Small handheld device uses sound waves to detect certain clinical laboratory biomarkers in blood samples
University of Colorado Boulder researchers have developed a novel technology that uses sound waves to test for biomarkers in blood samples. In addition to being very easy to use, the handheld device is portable, highly sensitive, and delivers results in minutes. Though not ready for clinical use, this is yet another example of how researchers are developing faster diagnostic tests that can be performed in near-patient settings, and which do not have to be done in core laboratories, shortening time to answer.
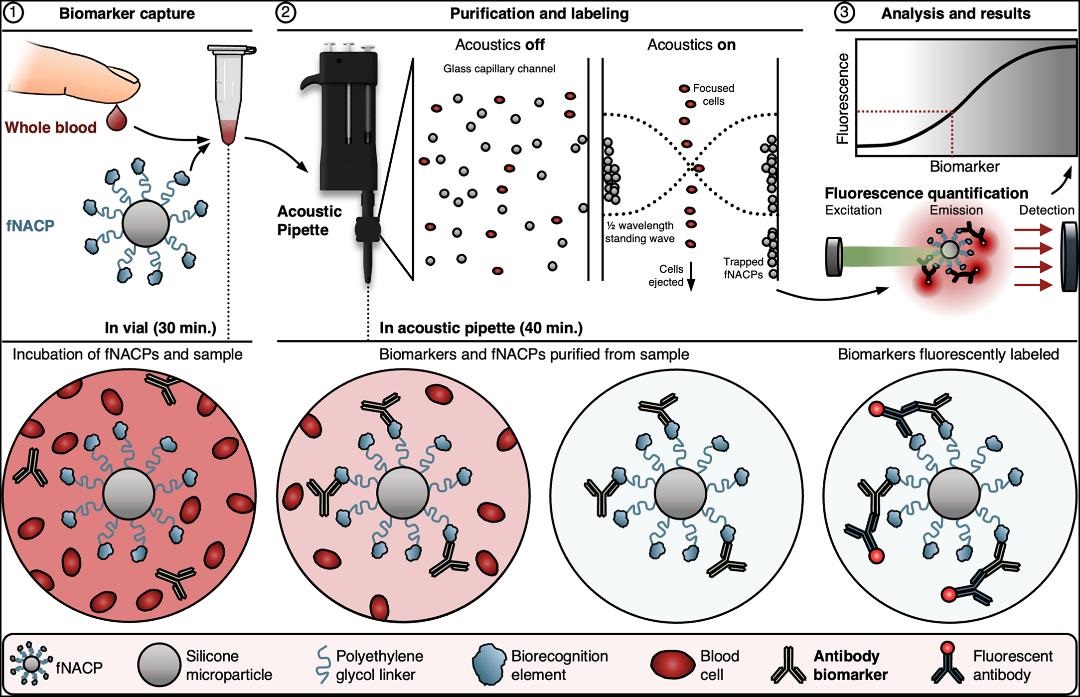
The small instrument—referred to as an “acoustic pipette”—delivers sound waves to tiny particles within the device called “functional negative acoustic contrast particles” (fNACPs). These particles are cell-sized balls that can be customized with different coatings to identify specific biomarkers—such as viruses or proteins—in tiny blood samples, according to a news release.
To operate the device, the custom fNACPs are mixed with a drop of blood and then placed inside the acoustic pipette. The mixture is then blasted with sound waves, which forces particles carrying certain biomarkers to one side of the chamber where they are trapped while the rest of the blood is expelled. The captured biomarkers are then labeled with fluorescent tags and examined with lasers to determine how much of a specific biomarker is present.
“We’re basically using sound waves to manipulate particles to rapidly isolate them from a really small volume of fluid,” said Cooper Thome (above), PhD candidate in Chemical and Biological Engineering at UC Boulder and first author of the study in a news release. “It’s a whole new way of measuring blood biomarkers,” he added. Should further studies validate this approach, clinical laboratories may be able to use this technology to perform diagnostic tests with smaller volumes of patient samples. (Photo copyright: University of Colorado Boulder.)
Blood Testing Quickly and in Multiple Settings
To test their invention, the UC Boulder researchers examined antibodies against a protein called ovalbumin, which is found in egg whites and often used in the development of various vaccines. The scientists discovered that their device could detect the antibodies even in low amounts.
Current rapid tests known as lateral-flow assays can detect specific biomarkers in blood or urine samples but cannot determine how much of the biomarker is present. Enzyme-linked immunotherapy assays (ELISA), the leading clinical laboratory blood test, requires expensive equipment and can take hours to days for results to be received.
With UC Boulder’s new handheld device, tiny blood samples collected from a single finger prick could ensure accurate test results are available quickly at the point of care as well as outside of traditional healthcare settings. This would greatly benefit people in developing nations and underserved communities and may help ease test anxiety for individuals who are apprehensive about traditional blood tests.
“We’ve developed a technology that is very user friendly, can be deployed in various settings, and provides valuable diagnostic information in a short time frame,” said Wyatt Shields IV, PhD, Assistant Professor, Department of Chemical and Biological Engineering, UC Boulder, and senior author of the research in the news release.
“In our paper, we demonstrate that this pipette and particle system can offer the same sensitivity and specificity as a gold-standard clinical test can but within an instrument which radically simplifies workflows,” he added. “It gives us the potential to perform blood diagnostics right at the patient’s bedside.”
The graphic above, taken from UC Boulder’s published paper, illustrates how “fNACPs capture target biomarkers from whole blood samples. fNACPs are purified from blood components by acoustic trapping and captured biomarkers are labeled with a fluorescent antibody within the acoustic pipette. fNACP fluorescence is then measured to determine biomarker presence and concentration.” (Graphic/caption copyright: University of Colorado Boulder.)
Not Like Theranos
The authors of the UC Boulder study are cognizant of some skepticism surrounding the field of biosensing, especially after the downfall of Theranos. The scientists insist their technology is different and based on systematic experiments and peer-reviewed research.
“While what they (Theranos) claimed to do isn’t possible right now, a lot of researchers are hoping something similar will be possible one day,” said Thome in the news release. “This work could be a step toward that goal—but one that is backed by science that anybody can access.”
The device is still in its initial proof-of-concept stage, but the UC Boulder scientists have applied for patents for the apparatus and are searching for ways to scale its use and expand its capabilities.
“We think this has a lot of potential to address some of the longstanding challenges that have come from having to take a blood sample from a patient, haul it off to a lab, and wait to get results back,” Shields noted.
More research, studies, and regulatory reviews will be needed before this technology becomes available for regular, widespread use. But UC Boulder’s new blood testing device is another example of a research team using novel technology to test for known biomarkers in ways that could improve standard clinical laboratory testing.
Best of all, the researchers say the test could provide an inexpensive means of early diagnosis. This assay could also be used to monitor how well patients respond to cancer therapy, according to a news release.
The protein had previously been identified as a promising biomarker and is readily detectable in tumor tissue, they wrote. However, it is found in extremely low concentrations in blood plasma and is “well below detection limits of conventional clinical laboratory methods,” they noted.
To overcome that obstacle, they employed an ultra-sensitive immunoassay known as a Simoa (Single-Molecule Array), an immunoassay platform for measuring fluid biomarkers.
“We were shocked by how well this test worked in detecting the biomarker’s expression across cancer types,” said lead study author gastroenterologist Martin Taylor, MD, PhD, Instructor in Pathology, Massachusetts General Hospital and Harvard Medical School, in the press release. “It’s created more questions for us to explore and sparked interest among collaborators across many institutions.”
“We’ve known since the 1980s that transposable elements were active in some cancers, and nearly 10 years ago we reported that ORF1p was a pervasive cancer biomarker, but, until now, we haven’t had the ability to detect it in blood tests,” said pathologist and study co-author Kathleen Burns, MD, PhD (above), Chair of the Department of Pathology at Dana-Farber Cancer Institute and a Professor of Pathology at Harvard Medical School, in a press release. “Having a technology capable of detecting ORF1p in blood opens so many possibilities for clinical applications.” Clinical laboratories may soon have a new blood test to detect multiple types of cancer. (Photo copyright: Dana-Farber Cancer Institute.)
Simoa’s Advantages
In their press release, the researchers described ORF1p as “a hallmark of many cancers, particularly p53-deficient epithelial cancers,” a category that includes lung, breast, prostate, uterine, pancreatic, and head and neck cancers in addition to the cancers noted above.
“Pervasive expression of ORF1p in carcinomas, and the lack of expression in normal tissues, makes ORF1p unlike other protein biomarkers which have normal expression levels,” Taylor said in the press release. “This unique biology makes it highly specific.”
Simoa was developed at the laboratory of study co-author David R. Walt, PhD, the Hansjörg Wyss Professor of Bioinspired Engineering at Harvard Medical School, and Professor of Pathology at Harvard Medical School and Brigham and Women’s Hospital.
The Simoa technology “enables 100- to 1,000-fold improvements in sensitivity over conventional enzyme-linked immunosorbent assay (ELISA) techniques, thus opening the window to measuring proteins at concentrations that have never been detected before in various biological fluids such as plasma or saliva,” according to the Walt Lab website.
Simoa assays take less than two hours to run and require less than $3 in consumables. They are “simple to perform, scalable, and have clinical-grade coefficients of variation,” the researchers wrote.
Study Results
Using the first generation of the ORF1p Simoa assay, the researchers tested blood samples of patients with a variety of cancers along with 406 individuals, regarded as healthy, who served as controls. The test proved to be most effective among patients with colorectal and ovarian cancer, finding detectable levels of ORF1p in 58% of former and 71% of the latter. Detectable levels were found in patients with advanced-stage as well as early-stage disease, the researchers wrote in Cancer Discovery.
Among the 406 healthy controls, the test found detectable levels of ORF1p in only five. However, the control with the highest detectable levels, regarded as healthy when donating blood, “was six months later found to have prostate cancer and 19 months later found to have lymphoma,” the researchers wrote.
They later reengineered the Simoa assay to increase its sensitivity, resulting in improved detection of the protein in blood samples from patients with colorectal, gastroesophageal, ovarian, uterine, and breast cancers.
The researchers also employed the test on samples from 19 patients with gastroesophageal cancer to gauge its utility for monitoring therapeutic response. Although this was a small sample, they found that among 13 patients who had responded to therapy, “circulating ORF1p dropped to undetectable levels at follow-up sampling.”
“More Work to Be Done”
The Simoa assay has limitations, the researchers acknowledged. It doesn’t identify the location of cancers, and it “isn’t successful in identifying all cancers and their subtypes,” the press release stated, adding that the test will likely be used in conjunction with other early-detection approaches. The researchers also said they want to gauge the test’s accuracy in larger cohorts.
“The test is very specific, but it doesn’t tell us enough information to be used in a vacuum,” Walt said in the news release. “It’s exciting to see the early success of this ultrasensitive assessment tool, but there is more work to be done.”
More studies will be needed to valid these findings. That this promising new multi-cancer immunoassay is based on a clinical laboratory blood sample means its less invasive and less painful for patients. It’s a good example of an assay that takes a proteomic approach looking for protein cancer biomarkers rather than the genetic approach looking for molecular DNA/RNA biomarkers of cancer.
ELISA tests at Icahn School of Medicine contradict earlier studies which found that antibodies developed to combat the SARS-CoV-2 coronavirus are short-lived
Medical laboratories at the forefront of the COVID-19 pandemic will be intrigued to learn that antibodies produced by the body to combat the coronavirus infection may actually provide long-term immunity, contrary to previous studies that found otherwise.
A recent study from the Icahn School of Medicine at Mount Sinai found that the protection may be more robust than previously believed. This may surprise many clinical laboratory scientists and clinical pathologists. Since the outbreak of the pandemic, multiple studies have been published with conflicting findings about the strength of the immune response to SARS-CoV-2 and the length of immunity provided after an infection.
In a Mount Sinai news release, however, Florian Krammer, PhD, microbiologist and Professor of Vaccinology in the Department of Microbiology at the Icahn School of Medicine at Mount Sinai, and a senior author of the paper, said, “While some reports have come out saying antibodies to this virus go away quickly, we have found just the opposite—that more than 90% of people who were mildly or moderately ill produce an antibody response strong enough to neutralize the virus, and the response is maintained for many months.”
The researchers published the findings of their study—which was based on an internally-developed antibody test—in Science.
The study concludes, “Although this cannot provide conclusive evidence that these antibody responses protect from reinfection, we believe it is very likely that they will decrease the odds ratio of reinfection and may attenuate disease in the case of breakthrough infection. We believe it is imperative to swiftly perform studies to investigate and establish a correlate of protection from infection with SARS-CoV-2.”
Florian Krammer, PhD (above), runs the Krammer Laboratory in the Department of Microbiology at the Icahn School of Medicine at Mount Sinai in New York. He noted that the longevity and neutralizing effects of antibody response are “critically important to enabling us to effectively monitor seroprevalence in communities, and to determining the duration and levels of antibody that protect us from reinfection.” Antibody response, he added, is also “essential for effective vaccine development.” (Photo copyright: Icahn School of Medicine at Mount Sinai.)
Details of the Icahn School of Medicine Study
The study arose from an effort by Mount Sinai to identify potential donors for a convalescent plasma therapy program. Beginning in late March, the health system used an enzyme-linked immunosorbent assay (ELISA) to screen thousands of individuals for presence of antibodies to the spike protein in the SARS-CoV-2 virus. The virus uses the spike protein to bind to a receptor in host cells, the researchers noted, making it “the main, and potentially only target for neutralizing antibodies.”
Screened patients either had confirmed cases of COVID-19, as determined by a polymerase chain reaction (PCR) test, or suspected cases, “defined as being told by a physician that symptoms may be related to SARS-CoV-2 or exposure to someone with confirmed SARS-CoV-2 infection,” the researchers wrote. The Mount Sinai health system also offered the test to employees.
Samples from each person were diluted in five discrete titers (concentrations) ranging from 1:80 to 1:2880, and each was tested for detectable presence of the antibodies. This allowed the researchers to categorize the samples as low, moderate, or high:
Low titers: 1:80 or 1:160
Moderate titers: 1:320
High titers: 1:960 or >1:2880
Between the start of the program and early October, the health system screened 72,401 people, of whom 30,082 tested positive for at least the lowest levels of antibodies. Among those who tested positive, a large majority fell into the moderate or high categories:
1:80: 690 (2.29%)
1:160: 1453 (4.83%)
1:320: 6765 (22.49%)
1:960: 9564 (31.79%)
1:2880: 11610 (38.60%)
The researchers also wanted to see whether the antibodies offered actual protection against the virus. So, they selected 120 samples and ran a quantitative microneutralization assay. In the lowest of the three categories, 50% of the samples showed neutralizing activity. That rose to 90% in the moderate category and 100% in the high category.
Finally, to determine how long protection might last, the researchers recalled 121 plasma donors for additional tests at two different points during the study. The researchers reported a slight drop in antibody levels about three months after onset of symptoms, and then a larger drop after five months. But antibodies were still present in most samples.
“It is still unclear if infection with SARS-CoV-2 in humans protects from reinfection and for how long,” the researchers wrote. “We know from work with common human coronaviruses that neutralizing antibodies are induced, and these antibodies can last for years and provide protection from reinfection or attenuate disease, even if individuals get reinfected.”
Previous ‘Conflicting’ Research
As previously noted, other studies raised doubts about the longevity of the antibodies produced by the body’s immune system. For example, the Mount Sinai researchers cited a study from China published in Nature Medicine that looked at the immune responses of 37 symptomatic patients and an equal number of asymptomatic individuals with laboratory-confirmed cases of the COVID-19 disease. In the latter group, 40% had no detectable levels of IgG antibodies after eight weeks.
The study also found a decrease in neutralizing antibodies in 30 of the asymptomatic individuals (81.1%) and 23 of the symptomatic individuals (62.2%) over the same period.
However, the Mount Sinai researchers pointed out that the antibody test in the Chinese study targeted a different protein. “The same paper also reported relatively stable (slightly declining) neutralizing antibody titers, which shows much higher concordance with our present findings,” they wrote. “Thus, the stability of the antibody response over time may also depend on the target antigen.”
A different study from England saw a 26% decline in antibodies over three months, CNN reported. That study, conducted by Imperial College London and Ipsos MORI, a market research firm, was based on responses from more than 365,000 randomly selected people who had self-administered a lateral flow antibody test.
But the seemingly conflicting studies from New York and the UK may not be contradictory, CNN reported. “People’s bodies produce an army of immune compounds in response to an infection and some are overwhelming at first, dying off quickly, while others build up more slowly. Measurements that show a waning antibody response in the first months after infection might be measuring this first wave—but there’s a second team building its forces in the background.”
In the same CNN report, Ania Wajnberg, MD, Director of Clinical Antibody Testing at Mount Sinai Hospital and co-author of the Icahn Mount Sinai study, said, “The serum antibody titer we measured in individuals initially were likely produced by plasmablasts—cells that act as first responders to an invading virus and come together to produce initial bouts of antibodies whose strength soon wanes.”
She added, “The sustained antibody levels that we subsequently observed are likely produced by long-lived plasma cells in the bone marrow. This is similar to what we see in other viruses and likely means they are here to stay. We will continue to follow this group over time to see if these levels remain stable as we suspect and hope they will.”
Does this mean that most people who get infected with the COVID-19 coronavirus will retain an immunity to the disease? Maybe. In the Icahn Mount Sanai study, Florian Kramer wrote, “More than 90% of people who were mildly or moderately ill produce an antibody response strong enough to neutralize the virus, and the response is maintained for many months.”
Thus, clinical laboratories engaged in serological testing may be asked to perform follow-up antibody tests to see if we do indeed create long-term immunity to COVID-19. Further, pathologists and medical laboratory scientists will want to follow future studies published in peer-reviewed journals to see if the findings of the Mount Sinai study are replicated at other sites.
The CDC and US Navy study reveals common symptoms and suggests best protective measures to prevent spread in enclosed environments that clinical labs and pathology groups could use to protect their staff members
Results from a study conducted by the US Navy and the federal Centers for Disease Control and Prevention (CDC) of sailors onboard the USS Theodore Roosevelt during the recent COVID-19 outbreak aboard the ship may be useful for pathologists and clinical laboratory managers. The study also provides public health and infectious disease specialists with an opportunity to learn more about how the SARS-CoV-2 coronavirus spreads in enclosed environments.
The aircraft carrier garnered headlines in April due to a widespread outbreak of the coronavirus among its crew. The investigators asked crewmembers to complete a questionnaire and provide samples for a serological antibody test and molecular diagnostics test, reported the Navy’s Bureau of Medicine and Surgery (BUMED). The goal was to learn more about the disease and how it spreads in high-density environments. The COVID-19 tests were conducted April 20-24 while the ship was docked in Guam.
“This study paints a picture of current and prior SARS-CoV-2 infection among young adults living in close quarters,” said the study’s lead author Dan Payne, PhD, an epidemiologist at the CDC, in the BUMED statement. “This data will contribute to understanding COVID-19 in the US military, as well as among young adults in other close communal environments.”
Participation in the study was voluntary. At the time of testing, a total of 1,417 service members were still on the ship or at the base in Guam, the researchers wrote in their study. Among them, 383 crewmembers agreed to complete the survey and provide a blood sample for an enzyme-linked immunosorbent assay (ELISA) antibody test. Out of that group, 267 also provided nasal swab samples for a reverse transcription polymerase chain reaction (RT-PCR) molecular diagnostic test.
A clinical laboratory team from the Naval Hospital Guam and the Navy and Marine Corps Public Health Center are seen above collecting surveys, nasal swabs, and blood samples from sailors assigned to the aircraft carrier USS Theodore Roosevelt (CVN 71) during the investigation into the COVID-19 outbreak in April. The ship’s medical leaders established an emergency command center, initiated a roving and deep cleaning team, and continually educated the crew on social distancing and proper protective procedures and behaviors, to mitigate the spread of the SARS-CoV-2 coronavirus. (Photo copyright: US Navy.)
The questionnaire sought information about sailors’ demographic factors, health history, symptoms, and preventive behaviors, such as mask wearing and physical distancing. Crewmembers who tested positive for reactive antibodies received an additional test to detect presence of neutralizing antibodies that inhibit the virus.
The median age of participants was 30 years. About 75% were male. Only 28 (7.3%) reported comorbidities such as a history of asthma, diabetes, hypertension, or immunosuppression, which are considered risk factors for developing serious cases of the COVID-19 disease.
Key findings of the CDC/Navy’s study:
228 participants (59.7%) tested positive for reactive antibodies. Of those, 135 (59.2%) tested positive for neutralizing antibodies.
235 participants had previously tested positive in a SARS-CoV-2 diagnostic test. Of those, 212 (90.2%) tested positive for reactive antibodies.
A total of 238 participants had a previous or current SARS-CoV-2 infection. Of these, 18.5% reported no symptoms.
Of the 194 sailors who reported symptoms, 115 (59.3%) sought medical care, and two were hospitalized.
The most frequently reported symptoms were headache (66.5%), loss of taste or smell or both (61.3%); myalgia (56.2%); runny nose (55.7%); and fatigue (55.2%).
The most effective preventive measures were avoidance of common areas, increased physical distancing, and use of face coverings.
“What we saw was that most of the infections were actually mild, in addition to those that were asymptomatic,” Payne told reporters after the study was published, reported CNN. “And this is perhaps different from studies of older Americans, or maybe even those who were hospitalized already, and certainly much different from those with underlying health conditions.”
But with the high number of asymptomatic cases, “symptom-based surveillance might not detect all infections,” noted the researchers, who cautioned that “the analysis was conducted on a convenience sample of persons who might have had a higher likelihood of exposure, and all information was based on self-report, raising the possibility of selection and recall biases.”
In January, the crew of the Roosevelt totaled about 4,800 sailors, reported Defense One. However, after docking in Guam, many sailors were moved to hotel rooms for quarantine. As of May 5, at least 1,156 crewmembers had tested positive for infection, Stars and Stripes reported, and one had died.
Sailors aboard the USS Theodore Roosevelt were examined prior to reboarding the ship following off-ship quarantine or isolation. Only those found to be negative for the coronavirus, were allowed to board the ship. (Photo copyright: US Navy.)
Impact of COVID-19 on the USS Theodore Roosevelt’s Crew
As of April 6, 172 crew members had tested positive for COVID-19, including the ship’s captain Brett Crozier. At that time, 61% of the crew had received clinical laboratory testing and 1,999 sailors had been moved off the ship into quarantine, reported Defense One. By the next day, 270 sailors tested positive, a 57% increase from the previous day.
By April 14, 589 crew members were diagnosed positive for COVID-19. With 92% of the crew tested, 3,922 were found to be negative for the infection. Nevertheless, 4,024 sailors—nearly 83% of the crew—were moved into isolation quarters off-ship to prevent spread of the coronavirus.
In their study, the Navy/CDC researchers concluded: “In this convenience sample of young, healthy US service members experiencing close contact aboard an aircraft carrier, those with previous or current SARS-CoV-2 infection experienced mild illness overall, and nearly 20% were asymptomatic. Approximately one third of participants reported fever, myalgia, and chills and had higher odds of SARS-CoV-2 infection than did persons who reported cough and shortness of breath. Participants reporting anosmia (loss of sense of smell) or ageusia (loss of sense of taste) had 10 times the odds of having infection, compared with those who did not.
“In this sample of intensely exposed subjects, assessed at a single point in time, results demonstrated that antibodies developed and that, at the time of specimen collection, many of these were neutralizing antibodies. … This is a promising indicator of immunity, and in several participants, neutralizing antibodies were still detectable >40 days after symptom onset. Ongoing studies assessing the humoral antibody response over time will aid the interpretation of serologic results in an outbreak investigation such as this.
“These results provide new indications of symptomatology of SARS-CoV-2 infections and serologic responses among a cohort of young US adults living in a congregate environment and contribute to a better understanding of COVID-19 epidemiology in the US military. The findings reinforce the importance of nonpharmaceutical interventions such as wearing a face covering, avoiding common areas, and observing social distancing to lower risk for infection in similar congregate living settings.”
Not all the specific lessons learned from this COVID-19 outbreak aboard a US Navy vessel will be applicable to clinical laboratories and anatomic pathology groups. Nevertheless, it is probable that the data gleaned from the CDC/Navy study aboard the USS Theodore Roosevelt will someday mean civilian Americans can count on improved responses to disease outbreaks from the nation’s testing laboratories.
Though experts say an antigen test is not as accurate as PCR tests, its low cost, ease of use, and widespread availability make it a boon for clinical labs performing COVID-19 testing
As former FDA commissioner Scott Gottlieb, MD, explained on Face the Nation, “this kind of technology is a real game changer … it’s a very rapid test that could be used in a doctor’s office. Doctors now have about forty thousand of these Sofia machines already installed in their offices … you do a simple nasal swab and the test itself scans for the antigens that the virus produces.
“The test is about 85% sensitive. So, let’s say a hundred people come into a doctor’s office who have COVID-19, eighty-five of them are going to be able to be tested positive with this test very quickly. It’s a cheap test. It’ll probably be about five dollars a test and you can get a result within five minutes … you’re getting a very fast result and you can start to take action immediately.
“The company itself said that they’re going to be able to produce about two hundred thousand of these tests starting right away. But in several weeks, they’ll be able to produce up to 1.5 million a week. So, this dramatically expands our testing capacity as long as doctors are able to run these tests in their offices.”
In an interview on CBS’ Face the Nation, former FDA Commissioner Scott Gottlieb, MD (above), said, “These antigen-based tests aren’t as reliable, meaning they’re not as sensitive. So, they’re going to miss some patients who have COVID. But in the hands of a doctor who already has a high index of suspicion that the patient may have the disease … they allow you to dramatically expand testing. And they’re very cheap. They’re very easy to perform. And again, most doctors have these machines already in their offices.” (Photo copyright: US Food and Drug Administration.)
Other LDTs That Have Received EUAs
Here’s a look at other laboratory-developed tests from major manufacturers that have received emergency-use authorizations from the FDA:
This test is designed for use with Abbott’s m2000 RealTime system, which is installed in about 200 US medical laboratories, the company says. It can run up to 470 patient samples in 24 hours. As of a May 11 statement, the company said it had shipped more than two million tests in the US.
This test is designed for use with Abbott’s Alinity m system, which the company describes as its “most advanced laboratory molecular instrument,” with the ability to run up to 1,080 tests in 24 hours, according to a press release.
This is a rapid test designed for use with the ID Now system, a compact portable instrument for point-of-care settings such as urgent care clinics. As of May 11, Abbott said it had shipped more than 1.7 million tests in the US, and that it planned to increase manufacturing capacity to two million tests per month.
However, the test has encountered some stumbling blocks. On May 14, the FDA issued an alert stating that the ID Now COVID-19 test could produce inaccurate negative results. This came after researchers at NYU Langone Health, Northwell Health, and Cleveland Clinic reported problems with the test, according to MedTech Dive. Abbott issued a statement suggesting that the problems were due to improper sample collection and handling, however, the FDA said that Abbott had agreed to conduct post-market studies to identify the cause of the false negatives and suggest remedial actions.
This is a qualitative test designed to detect the presence of IgG antibodies following a SARS-CoV-2 infection. The FDA authorized use of the assay on Abbott’s Architect i2000SR system in April, and then followed up with a May 11 EUA for its use on the Alinity i system. In a statement, Abbott said it planned to ship 30 million tests globally starting in May.
In a March statement, the FDA touted this as the first point-of-care COVID-19 test to receive an EUA. The company estimates the detection time as approximately 45 minutes. It is designed for use with Cepheid’s GeneXpert Dx diagnostic software and GeneXpert Infinity systems, which have nearly 5,000 US installations, according to a Cepheid statement.
This test runs on Hologic’s Panther system, which, according to a Hologic press release, can provide results in about three hours and run more than 1,000 tests per day. The company claims that more than 1,000 Panther systems are installed in US labs, and that it expects to produce an average of one million tests per week.
Ortho’s antibody test is designed for use with its VITROS XT 7600, 3600, 5600, and ECi/ECiQ immunodiagnostic systems, which, the company says are installed in more than 1,000 US labs. The Total Reagent Pack is a qualitative test that detects the presence of all antibodies against SARS-CoV-2.
On April 24, Ortho announced it had received another FDA EUA, this one for its Anti-SARS-CoV-2 IgG test, which detects the presence of IgG antibodies. In a statement, the company said it expects to produce “several million” IgG tests per month.
This test is designed for use with Roche’s cobas 6800 and 8800 systems. The 6800 can process up to 384 results in an eight-hour shift, Roche says, compared with 1,056 results for the 8800 model. The company says results are available in about 3.5 hours. In a statement, Roche said it planned to ship 400,000 tests per week.
Roche describes this as a qualitative antibody test that can be used on cobas e series immunoassay analyzers. Testing time is 18 minutes. As of May 19, the test was live at more than 20 US labs, “with plans in the next several weeks to increase to more than 200 commercial and hospital lab sites with the ability to perform millions of tests per week,” the company stated in a press release.
It’s likely the FDA will continue to issue emergency-use authorizations as the agency receives more applications from IVD manufacturers.