Trifecta of forces at work that will affect the clinical laboratory and pathology industries have been described as a ‘perfect storm’ requiring lab and practice managers to be well informed
Digital pathology, artificial intelligence (AI) in healthcare, and the perfect storm of changing federal regulations, took centerstage at the 29th Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management in New Orleans this week, where more than 1,000 clinical laboratory and pathology leaders convened over three days.
This was the largest number of people ever onsite for what has become the world’s largest event focused exclusively on lab management topics and solutions. Perhaps the highlight of the week was the federal Food and Drug Administration’s (FDA’s) announcement of its final rule on Laboratory Developed Tests (LDTs). Overall, the conference featured more than 120 speakers, many of them national thought leaders on the topic of clinical lab and pathology management. More than 65% of the audience onsite were executive level lab managers.
“The level of interest in the annual Executive War College is testimony to the ongoing need for dynamic, engaging, and highly relevant conference events,” said Robert Michel (above), Editor-in-Chief of Dark Daily and its sister publication The Dark Report, and founder of the Executive War College. “These in-person gatherings present great opportunities for clinical laboratory and pathology managers and leaders to network and speak with people they otherwise might not meet.” (Photo copyright: Dark Intelligence Group.)
Demonstrating Clinical Value
For those who missed the action onsite, the following is a synopsis of the highlights this week.
Lâle White, Executive Chair and CEO of XiFin, spoke about the future of clinical laboratory testing and the factors reshaping the industry. There are multiple dynamics impacting healthcare economics and outcomes—namely rising costs, decreasing reimbursements, and the move to a more consumer-focused healthcare. But it is up to labs, she said, to ensure their services are not simply viewed as a commodity.
“Laboratory diagnostics have the potential to change the economics of healthcare by really gaining efficiencies,” she noted. “And it’s up to labs to demonstrate clinical value by helping physicians manage two key diagnostic decision points—what tests to order, and what to do with the results.”
But even as labs find ways to increase the value offered to clinicians, there are other disruptive factors in play. Consumer-oriented tech companies such as Google, Apple, and Amazon are democratizing access to patient data in unforeseen ways, and Medicare Advantage plans are changing the way claims are processed and paid.
Clinical labs are fundamental components of the public health infrastructure. So, the CDC plans on focusing on delivering high-quality laboratory science, supported by reliable diagnostics and informatics for disease outbreaks and exposures, and engaging with public and private sector partners.
The history of MolDX and Z-Codes were the topics discussed by Gabriel Bien-Willner, MD, PhD, Chief Medical Officer for healthcare claims and transaction processing company Palmetto GBA. Molecular testing is highly complex, and the lack of well-defined billing codes and standardization makes it difficult to know if a given test is reasonable and necessary.
Z-Codes were established to clarify what molecular testing was performed—and why—prompting payers to require both Z-Codes and Current Procedural Terminology (CPT) codes when processing molecular test claims. Medicare’s MolDX program further streamlines the claims process by utilizing expertise in the molecular diagnostics space to help payers develop coverage policies and reimbursement for these tests.
FDA Final Rule on LDT Regulation
Timothy Stenzel, MD, PhD, CEO of Grey Haven Consulting and former director of the FDA’s Office of In Vitro Diagnostics reviewed the latest updates from the FDA’s Final Rule on LDT (laboratory developed test) regulation. Prior to the FDA releasing its final rule, some experts suggested that the new regulations could result in up to 90% of labs discontinuing their LDT programs, impacting innovation, and patient care.
However, the final rule on LDTs is very different from the original proposed rule which created controversy. The final rule actually lowers the regulatory burden to the point that some labs may not have to submit their LDTs at all. The FDA is reviewing dozens of multi-cancer detection assays, some of which have launched clinically as LDTs. The agency is likely to approve those that accurately detect cancers for which there is no formal screening program.
Stenzel explained the FDA’s plan to down-classify most in vitro diagnostic tests, changing them from Class III to Class II, and exempting more than 1,000 assays from FDA review. He also discussed the highlights of the Quality Management System Regulation (QMSR). Launched in January, the QMSR bought FDA requirements in line with ISO 13485, making compliance easier for medical device manufacturers and test developers working internationally.
Looming Perfect Storm of Regulatory Changes
To close out Day 1, Michel took to the stage again with a warning to clinical laboratories about the looming “Perfect Storm” trifecta—the final FDA ruling on LDTs, Z-Code requirements for genetic testing, and updates to CLIA ’92 that could result in patient data being considered a specimen.
Laboratory leaders must think strategically if their labs are to survive the fallout, because the financial stress felt by labs in recent years will only be exacerbated by macroeconomic trends such as:
Staff shortages,
Rising costs,
Decreasing and delayed reimbursements, and
Tightening supply chains.
Lab administrators looking for ways to remain profitable and prosperous should look beyond the transactional Clinical Lab 1.0 fee-for-service model and adopt Clinical Lab 2.0, which embraces HEDIS (Healthcare Effectiveness Data and Information Set) scores and STAR ratings to offer more value to Medicare Advantage and other payers.
Wednesday’s General Session agenda was packed with information about the rise of artificial intelligence, big data, and precision medicine in healthcare. Taking centerstage on the program’s final day was Michael Simpson, President and CEO of Clinisys. Simpson gave a global perspective on healthcare data as the new driver of innovation in diagnostics and patient care.
Switching from non-profit to for-profit may affect how clinical laboratories operate in the new healthcare system
Shifting away from fee-for-service payment models and towards value-based healthcare is the goal of many non-profit hospital systems. One such transformation is underway at Summa Health, one of the largest integrated delivery networks (IDNs) in Ohio. On January 17, venture capital firm General Catalyst announced that its subsidiary—Health Assurance Transformation Corporation (HATCo)—had entered into an agreement to purchase Summa Health.
“HATCo’s investment into Summa Health will drive not only near-term benefit to the organization and the patients it serves but also sustainable, long-term transformation through a true shift to value-based care and access to new revenue streams, resources, innovations, and technologies,” states a General Catalyst news release penned by Marc Harrison, MD, CEO of HATCo.
Harrison was formerly President and CEO of Intermountain Healthcare, a 33 hospital not-for-profit IDN in Salt Lake City, Utah. This is a noteworthy fact because Intermountain Health has a national reputation as an innovative multi-hospital health system. Some observers believe that Harrison’s involvement signals that General Catalyst believes it has a care model that can deliver better patient care in a profitable manner.
“Under its new structure, Summa will become a for-profit organization, and General Catalyst says it will introduce new tech-enabled solutions that aim to make care more accessible and affordable,” CNBCreported.
“This is the first time that anybody has done anything quite like this,” Harrison told CNBC. “There are many digital health solutions that are out there as point solutions. This is the first holistic transformation of a health system to a thoughtful combination of digital and in-person care.”
“Our intent is to build on and augment the system’s considerable strengths. First and foremost, we share Summa Health’s commitment to serving all members of the community,” wrote HATCo CEO Marc Harrison, MD (above), in a news release. “The Summa Health team also shares our belief that achieving healthcare transformation will require a shift to value-based care … Together, we intend to demonstrate that a model that is better for patients can also be good for business, creating a blueprint for other health systems to effectively serve all people in their communities.” How this shift will affect Summa’s clinical laboratories remains to be seen. (Photo copyright: General Catalyst.)
Betting on Healthcare
In 2023, General Catalyst, an American venture capital firm headquartered in Cambridge, Mass., unveiled its Health Assurance Transformation Corporation (HATCo) and began shopping for a health system to buy.
HATCo has 20 healthcare systems in a network that spans 43 states and four countries, according to Healthcare Dive. The company’s news release states it has been focused on three areas since its start-up:
Helping its partners on their “transformation journeys.”
Planning to “acquire and operate a health system for the long-term.”
“The goal of the purchase is for the health system to act as a proving ground for General Catalyst to test ways to improve hospital operations and patient care, without risk aversion or cash shortfalls, management said,” Healthcare Dive reported.
Thus, the firm’s announcement to purchase a health system last October “sent shockwaves through the healthcare industry” according to Healthcare Dive.
“At its core, General Catalyst’s long-term Health Assurance thesis is that value-based care not only is good for patients, but also can be a successful business model if deployed with innovative technology at meaningful scale. Its rationale for buying a health system is a belief that it can improve on the traditional model of not-for-profit health system governance and management by embedding new incentives,” wrote Christopher Kerns, CEO and co-founder of Washington, D.C-based research firm Union Healthcare Insight, in a blog post analysis.
General Catalyst’s HATCo may offer up “a profit motive, a longer time horizon, and a channel for dozens of innovative companies to demonstrate value,” he noted.
“The single biggest barrier to promising young healthcare companies is an inability to scale. Many of their innovations—in digital health, patient engagement, revenue cycle workflow, etc.—require willing health system partners who are famously conservative in their investments and service providers, and rarely take risks on newbies. The addition of Summa provides an open laboratory for those innovations,” Kerns added.
Is the Summa Health Deal Good for Healthcare?
Some in the industry were taken aback by General Catalyst’s announcement.
“A lot of people feel like a PE (private equity) or venture capital company owning a hospital is kind of like asking Freddy Krueger to come babysit your kids. It just makes people a little nervous, and it doesn’t feel quite aligned with this concept of healthcare being a human right,” John Bass, CEO of Hashed Health, a Nashville, Tenn.-based healthcare venture studio, told CNBC.
Nevertheless, it’s a moot point. HATCo is moving forward with its purchase of Summa Health.
“For this bet to work, Summa will have to be a solid proving ground for [General Catalyst’s] portfolio companies. And that means either Summa itself will have to grow, or it will have to act as a force multiplier for its other value-based portfolio companies to justify the considerable capital expended. I have to say, that’s a tall order, but not an insane one,” said Kerns in the Union Healthcare Insight blog post.
Healthcare managers may find it interesting to follow HATCo and Summa Health on their planned journey. The results may speak for themselves. Either way, clinical laboratories and anatomic pathology group practices in HATCo’s health system may be in for some interesting changes.
From ‘new-school’ rules of running a clinical laboratory to pharmacy partnerships to leveraging lab data for diagnostics, key industry executives discussed the new era of clinical laboratory and pathology operations
Opening keynotes at the 28th Annual Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management taking place in New Orleans this week covered three main forces that healthcare and medical laboratory administrators should be preparing to address: new consumer preferences, new care models, and new payment models.
“COVID-19 didn’t change a whole lot of things in one sense, but it accelerated a lot of trends that were already happening in healthcare,” said Robert L. Michel, Editor-in-Chief of Dark Daily and its sister publication The Dark Report, and Founder of the Executive War College, during his opening keynote address to a packed ballroom of conference attendees. “Healthcare is transforming, and the transformation is far more pervasive than most consumers appreciate.
“Disintermediation, for example, is taking traditional service providers and disrupting them in substantial ways, and if you think about the end of fee-for-service, be looking forward because your labs can be paid for the value you originate that makes a difference in patient care,” Michel added.
Another opportunity for clinical laboratories, according to Michel, is serving Medicare Advantage plans which have soared in enrollment. “Lab leaders should be studying Medicare Advantage for how to integrate Medicare Advantage incentives into their lab strategies,” he said, highlighting the new influence of risk adjustment models which use diagnostic data to predict health condition expenditures.
Opening sessions at this week’s annual Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management, presented by Robert L. Michel (above), Editor-in-Chief of Dark Daily and its sister publication The Dark Report, discussed demand for delivering healthcare services—including medical laboratory testing—as consumer preferences evolve, new care models are designed, and as payers seek value over volume. While these three forces may be challenging at the outset, they also create opportunities for clinical laboratories and pathology groups—a focal point of the Executive War College each year. (Photo copyright: The Dark Intelligence Group.)
Medical Laboratories Must Adapt to ‘New-School’ Rules
During his keynote address, Stan Schofield, Vice President and Managing Principal at The Compass Group, noted that while the basic “old-school” rules of successfully running a clinical laboratory have not changed—e.g., adding clients, keeping clients, creating revenue opportunities, getting paid, and reducing expenses—the interpretation of each rule has changed. The Compass Group is a trade federation based in South Carolina that serves not-for-profit healthcare integrated delivery networks (IDNs), including 32 health systems and 600 hospitals.
Schofield advised that when it comes to adding new clients under the “new-school” rules of lab management, clinical laboratory directors must be aware of and adapt to hospital integrations of core labs, clinical integrations across health systems, seamless services, direct contracting with employers in insurance relationships, and direct-to-consumer testing. Keeping clients, Schofield said, involves five elements:
Strong customer service.
A tailored metrics program for quality services based on what is important to a lab’s clients.
Balanced scorecards that look at the business opportunity and value proposition with each client.
Monitoring patients’ experiences and continuous improvement.
Participation in all payer agreements.
As to the problem of commoditization of laboratory goods and services, Schofield said, “Right now, we’re facing the monetization of the laboratory. We’re going to swiftly move from commoditization to monetization to commercialization.”
Pharmacies Enter the Clinical Laboratory Market
In another forward looking keynote address, David Pope, PharmD, CDE, Chief Pharmacy Officer at OmniSYS, XiFin Pharmacy Solutions, discussed the “test to treat” trend which could bring clinical laboratories and pharmacies together in new partnerships.
Diagnostics and pharmacy now intersect, according to Pope. “Pharmacists are on the move, and they are true contender as a new provider for you,” he said. “An area of pharmacy that is dependent upon labs is specialty medications.”
Specialty medicines now account for 55% of prescription spending, up from 28% in 2011, driven by growth in auto-immune and oncology, Pope noted. Other examples include companion diagnostics required for targeted treatments pertaining to all major cancers, and new areas like thalassemia (inherited blood disorders), obesity, next-generation sequencing, and pharmacogenomics, in addition to routine testing such as liver function and complete blood count (CBC).
Federal legislation may soon recognize pharmacists as healthcare providers who will be trained to perform specific clinical services, Pope said. Some states already recognize pharmacists as providers, he noted, explaining that pharmacies need lab data for three primary reasons:
Service—Pharmacies can act as a referral source to clinical laboratories. When referring, pharmacies may need to communicate lab test results to patients or providers to coordinate care.
Value-based care—Pharmacies would draw on data to counsel, prescribe, and coordinate care for chronic disease management, among other services.
Diagnostics and pharmacogenetics—Specialty medication workflows require documented test results within a specific timeframe prior to dispensing.
Another point Pope made: Large pharmacies are seeking lab partners. Labs that can provide rapid turnaround time and good pricing on complex tests provide pharmacies with partnership opportunities.
Using AI to Create Patients’ ‘Digital Twins’ That Help Identify Disease and Improve Care
High-tech healthcare technology underlies many opportunities in the clinical laboratory and pathology market, as evidenced throughout the Executive War College’s 2023 curriculum. An ongoing challenge for labs, however, is how to produce the valuable datasets that all labs have the potential to generate.
“It feels like we’ve come so far,” explained Brad Bostic, CEO of hc1 during his keynote address. “We’ve got the internet. We’ve got the cloud. All of this is amazing, but in reality, we have this massive proliferation of data everywhere and it’s very difficult to know how to actually put that into use. And nobody’s generating more data than clinical laboratories.
“Every single interaction with a patient that generates data gives you this opportunity to create the idea of a ‘digital twin.’ That means that labs are creating a mathematical description of what a person’s state is and using that information to look at how providers can optimally diagnose and treat that person. Ultimately, it is bigger than just one person. It’s hundreds of millions of people that are generating all this data, and many of these people fall into similar cohorts.”
This digital twin opportunity is heavily fueled by medical laboratory testing, Bostic said, adding that labs need to be able to leverage artificial intelligence (AI) to:
“I recommend lab leaders sit down with their teams and any outside partners they trust and identify what are their lab’s goals,” Bostic stated. “Think about how this technology can advance a lab’s mission. Look at strategy holistically—everything from internal operations to how patient care is affected.”
Medical laboratories and anatomic pathologists may need to squeeze into narrow networks to be paid under value-based schemes, especially where Medicare Advantage is concerned
Pathologists have likely heard the arguments in favor of value-based payment versus fee-for-service (FFS) reimbursement models: FFS encourages providers to order medically unnecessary procedures and lab tests. FFS removes incentives for providers to order patient services more carefully. Fraudsters can generate huge volumes of FFS claims that take payers months/years to recognize and stop.
Studies that favor value-based payment schemes support these claims. But do hospitals and other healthcare providers also accept them? And how is value-based reimbursement really doing?
To find out, Chicago-based thought leadership and advisory company 4Sight Health culled data from various organizations’ reports that suggest value-based reimbursement shows signs of growth as well as signs of stagnation.
Value-Based Payment Has Its Ups and Downs
Healthcare journalist David Burda is News Editor and Columnist at 4Sight Health. In his article, “Is Value-Based Reimbursement Mostly Dead or Slightly Alive?” Burda commented on data from various industry reports that indicated value-based reimbursement shows “signs of life.” For example:
More doctors are accepting pay-for-performance payments: 44.5% in 2020, up from 42.3% in 2018, according to an American Medical Association (AMA) biennial report on physician participation in value-based reimbursement, titled, “Policy Research Perspectives: Payment and Delivery in 2020.”
On the other hand, Burda reported that value-based reimbursement also has these declining indicators:
39.3% of provider payments “flowed” through FFS plans in 2020 with no link to cost or quality. This was unchanged since 2019. (HCPLAN report)
19.8% of FFS payments to providers in 2020 were linked to cost or quality, down from 22.5% in 2019. (HCPLAN report)
88% of doctors reported accepting FFS payments in 2019, an increase from 87% in 2018. (AMA report)
Does Today’s Healthcare Industry Support Value-based Care?
A survey of 680 physicians conducted by the Deloitte Center for Health Solutions suggests the answer could be “not yet.” In “Equipping Physicians for Value-Based Care,” Deloitte reported:
“Physician compensation continues to emphasize volume more than value.
“Availability and use of data-driven tools to support physicians in practicing value-based care continue to lag.
“Existing care models do not support value-based care.”
Deloitte analysts wrote, “Physicians increasingly recognize their role in improving the affordability of care. We repeated a question we asked six years ago and saw a large increase in the proportion of physicians who say they have a prominent role in limiting the use of unnecessary treatments and tests: 76% in 2020 vs. 57% in 2014.
“Physicians also recognize that today’s care models are not geared toward value,” Deloitte continued. “They see many untapped opportunities for improving quality and efficiency. They estimate that even today, sizable portions of their work can be performed by nonphysicians (30%) in nontraditional settings (30%) and/or can be automated (18%), creating opportunities for multidisciplinary care teams and clinicians to work at the top of their license.”
Hospital CFOs Also See Opportunities for Value-based Care
This could be problematic for clinical laboratories, according to Robert Michel, Editor-in-Chief of Dark Daily and our sister publication The Dark Report. According to Guidehouse, “Nearly 60% of health systems plan to advance into risk-based Medicare Advantage models in 2022.”
Medicare Advantage (MA) enrollments have escalated over 10 years: 26.4 million people of the 62.7 million eligible for Medicare chose MA in 2021, noted a Kaiser Family Foundation brief that also noted MA enrollment in 2021 was up by 2.4 million beneficiaries or 10% over 2020.
The graph above is taken from the Kaiser Family Foundation report, “Medicare Advantage in 2021: Enrollment Update and Key Trends.” According to the KFF, “In 2021, more than four in 10 (42%) Medicare beneficiaries—26.4 million people out of 62.7 million Medicare beneficiaries overall—are enrolled in Medicare Advantage plans; this share has steadily increased over time since the early 2000s.” Since MA employs narrow networks for its healthcare providers, it’s likely this trend will continue to affect clinical laboratories that may find it difficult to access these providers. (Graphic copyright: Kaiser Family Foundation.)
“The shift from Medicare Part B—where any lab can bill Medicare on behalf of patients for doctor visits and outpatient care, including lab tests—to Medicare Advantage is a serious financial threat for smaller and regional labs that do a lot of Medicare Part B testing. The Medicare Advantage plans often have networks that exclude all but a handful of clinical laboratories as contracted providers,” Michel cautioned. “Moving into the future, it’s incumbent on regional and smaller clinical laboratories to develop value-added services that solve health plans’ pain points and encourage insurers to include local labs in their networks.”
Medical laboratories and anatomic pathology groups need to be aware of this trend. Michel says value-based care programs call on clinical laboratories to collaborate with healthcare partners toward goals of closing care gaps.
“Physicians and hospitals in a value-based environment need a different level of service and professional consultation from the lab and pathology group because they are being incented to detect disease earlier and be active in managing patients with chronic conditions to keep them healthy and out of the hospital,” he added.
Value-based reimbursement may eventually replace fee-for-service contracts. The change, however, is slow and clinical laboratories should monitor for opportunities and potential pitfalls the new payment arrangements might bring.
Demographic shifts are most acute in Europe and East Asia but could be a harbinger of things to come for US healthcare as well
Across the globe, major shifts in many countries’ demographics are starting to drive notable changes in how healthcare is delivered in these nations. Having fewer pediatric patients and more senior citizens is fundamentally altering what types of tests are in greatest demand from the medical laboratories in these countries. It is the population trend writ large on a global scale.
For example, in countries as diverse as Sweden, Hungary, Japan, and South Korea, birthrates are declining as fewer young people decide to have kids, or they choose to have smaller families. Thus, demand for pediatric care is declining in those countries.
Meanwhile, populations around the world continue to age as greater numbers of people reach their retirement years. Not only does this create the need to expand medical services designed to serve the elderly, but there are important economic consequences. That’s because each wave of retirees leaves fewer people in the workforce to support the healthcare of ever-growing numbers of senior citizens.
According to The New York Times (NYT), this trend is likely to accelerate. In “Long Slide Looms for World Population, with Sweeping Ramifications,” the paper reported that “All over the world, countries are confronting population stagnation and a fertility bust, a dizzying reversal unmatched in recorded history that will make first-birthday parties a rarer sight than funerals, and empty homes a common eyesore.”
The NYT added that, “With fewer births, fewer girls grow up to have children, and if they have smaller families than their parents did—which is happening in dozens of countries—the drop starts to look like a rock thrown off a cliff.”
In countries such as the US, Canada, and Australia, this is partially mitigated by immigration, the NYT reports. However, some nations, such as Germany and South Korea, have instituted programs aimed at boosting birthrates, though with varying degrees of success.
According to demographer Frank Swiaczny, Dr. rer. nat., Senior Research Fellow at the Federal Institute for Population Research in Germany, countries around the world—especially in Europe and East Asia—“need to learn to live with and adapt to decline.”
“A paradigm shift is necessary,” he told the NYT.
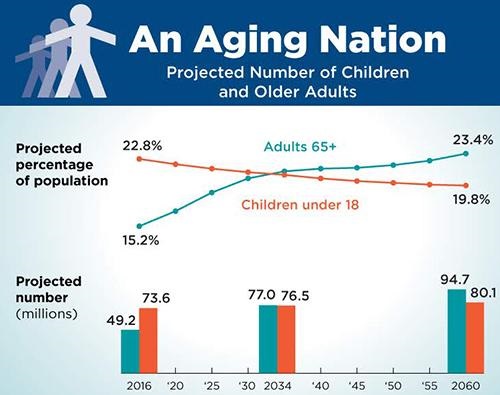
The graphic above, taken from the US Census Bureau’s 2018 report, “The Graying of America: More Older Adults than Kids by 2035,” illustrates the rate at which America’s elder population is catching up with the rest of the world. It will soon exceed younger portions of the population, thus shifting demand for healthcare from pediatrics to geriatrics. Anatomic pathology groups and clinical laboratories will be impacted by this trend. (Graphic copyright: US Census Bureau.)
The authors, which included Terry Fulmer PhD, RN, FAAN, and John Auerbach, Director of Intergovernmental and Strategic Affairs at the CDC, noted that in 2018, adults 65 or older were 15.6% of the population. This will rise to 20% by 2030, when, according to the authors, seniors will outnumber the portion of the population that is younger than age five.
Foster an “expanded and better-trained workforce” to care for older adults, through enhanced training as well as “scholarships, loan forgiveness, and clinical internships.”
Adapt the public health system to account more for the needs of an aging population, such as by “improved coordination and collaboration with Area Agencies on Aging and key healthcare providers.”
Address disparities and inequities in healthcare access, such as social isolation “caused or exacerbated by social, economic, and environmental conditions.”
Facilitate advances in telehealth and other technologies to improve care delivery. “The lack of access to technology, low digital health literacy, and design barriers in patient portals and apps have disproportionately affected older adults, especially those in underserved communities,” the authors wrote.
Improve palliative and end-of-life care. “Many older adults are living with serious illness,” the authors wrote, and “most will live for years with their illnesses, resulting in a high burden of physical and psychological distress, functional dependence, poor quality of life, high acute care use, loss of savings, and caregiver distress.”
Reform long-term care, by improving conditions in long-term care facilities and making it easier for older adults to stay at home.
A perspective in the journal NPJ Urban Sustainability, titled “Ageing and Population Shrinking: Implications for Sustainability in the Urban Century,” notes that these trends have led some cities or countries to adopt technological innovations in healthcare, such as “socially assistive robots and virtual entertainment for mental health, roadside AI services for healthcare, and a series of innovations for house-based healthcare, digital nursing, and monitoring.”
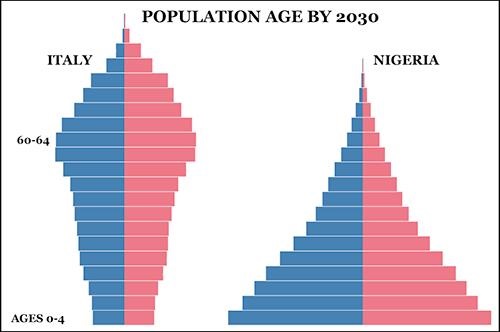
The graphic above, taken from PopulationPyramid.net, illustrates the stark differences in the age of populations in two countries at opposite ends of the progressing demographic shift. Italy’s population pyramid (left) shows how the senior population makes up a substantial proportion of total population, while Nigeria’s 2030 population pyramid (right) shows the classic pyramid of a wide base of younger people trailing off to a small number of the elderly at the top of the pyramid. Medical laboratories in those nations will continue to be affected by how these demographic shifts taking place worldwide are changing the type of healthcare in highest demand. (Graphic copyright: PopulationPyramid.net.)
Impact on Pediatrics
At the other end of the age spectrum, a recent presentation from the American Academy of Pediatrics noted a 13% decline in the US birthrate between 2007 and 2019. But a white paper from physician search firm Merritt Hawkins suggests this has not necessarily resulted in reduced demand for pediatric services, at least not in the US.
Despite the decline, “there are still about four million births in the US annually, and immigration adds to the number of children in the population,” the white paper notes. Even rural areas with aging populations “have far fewer pediatricians per capita than they require.”
However, according to The New York Times, in South Korea, “expectant mothers in many areas can no longer find obstetricians or postnatal care centers.” And the town of Agnone, Italy, no longer has a maternity ward because the number of births—just six this year—is below the national minimum.
This is important to note. If there are developed countries around the world where demographics point to a steady decline in population, then the type of healthcare provided will be different than what is currently used. Clinical laboratories and pathology groups in those regions can expect changes and should prepare for them.