Clinical laboratories and pathology groups can benefit from knowing how genetic testing is being used for other than medical testing purposes
It is useful for pathologists and clinical laboratory managers to be aware of the different ways genetic testing and DNA sequencing is being conducted. That’s because a genetic test for one purpose—such as identifying an individual’s relatives and connection to a region or a cultural group—might generate data that could become part of that person’s medical care.
Thus, an ongoing genetic study in South Africa highlighting the issue of so-called “helicopter research” will be informative for Dark Daily’s readers.
Also known as “neo-colonial science,” helicopter research describes when scientists from wealthy countries perform research in lower-income countries in ways that may be deemed exploitative or disrespectful to local populations.
“Scientists conduct helicopter research when they collect data from developing countries and marginalized communities with little to no involvement from local researchers and community members,” wrote researchers Dana Al-Hindi, and Brenna Henn PhD, in an article for The Conversation. “Helicopter research also occurs when researchers take data out of the country they collected it from without either providing benefit to or sharing the results with the community.”
In an article for The Conversation, UC Davis researchers Brenna Henn, PhD (left), and Dana Al-Hindi (right), wrote, “While we have learned a great deal from these communities, we have been unable to fulfill a common request: providing them their individual genetic ancestry result. In our attempts to overcome the logistical challenges of providing this information, we’ve grappled with the common question of how to ensure an equitable balance of benefits between researchers and the community they study. What we’ve found is that there is no easy answer.” Clinical laboratories will want to remember the term “Helicopter Research” in relation to these types of studies. (Photos copyright: UC Davis/The Conversation.)
The South Africa study, conducted over the past 12 years, aims to use genetic data “to help unravel the history and prehistory of southern Africans and their relationship to populations around the world,” the authors wrote in The Conversation.
The researchers have been using the genetic data to trace the ancestry of indigenous Khoekhoe and San peoples in South Africa as well as other populations that self-identify as “Colored.”
“Early European colonizers initially used this term to refer to indigenous Khoekhoe and San groups long before it was codified by the apartheid government in 1948,” the researchers wrote. “It persists today as an ethnic category, broadly encompassing Khoe-San groups, various East African, Indian, and Southeast Asian populations brought by the slave trade, and people of mixed ancestry.”
Challenges Sharing Genetic Data with Study Participants
Participants in the study have asked to see their personal genetic ancestry results, but the researchers noted several challenges, including local restrictions and the difficulty of presenting complex data in “an accessible and digestible form.” So, the researchers partnered with consumer-focused genetic testing company 23andMe (NASDAQ:ME).
23andMe provided additional funding for the research, assisted the researchers in community outreach, and “expanded our ability to ‘capacity-build’—that is, to make sure that the knowledge and skills we gain are shared with local institutions,” Henn and Al-Hindi wrote in The Conversation. They added that they are still dealing with questions about whether their efforts to provide equitable benefits are sufficient.
“Our research team, local collaborators, and 23andMe are all concerned about how to best address the risk of helicopter research, coercion, and any unknown risks that may arise from disclosing personal ancestry results,” they wrote.
Cape Town Statement on Fostering Research Integrity
The issue of helicopter research was a major focus at the 7th World Conference on Research Integrity (WCRI), held May 29-June 1 in Cape Town, South Africa. It was the first WCRI to be held in Africa and adopted the theme “Fostering Research Integrity in an Unequal World.”
One outcome of the conference will be an effort to produce what is known as the Cape Town Statement on Fostering Research Integrity. The statement will “highlight the importance of fairness in international research partnerships,” noted Research Professional News.
The statement “compels institutions and researchers alike to act on their responsibilities to promote equity, diversity, and fairness in research partnerships,” conference speaker Retha Visagie, DCur, told the publication. She leads the Research Integrity Office at the University of South Africa.
Conference co-chair Lyn Horn, PhD, director the Office of Research Integrity at the University of Cape Town, told the publication that it could take up to a year before a draft of the statement is ready for comment.
One overarching goal will be to “demonstrate why inequity and unfair practices in research collaborations and contexts is a research integrity (RI) matter,” the authors wrote. “Second it must identify some key values or principles and action guides that will address the issue of equity and fairness in research within the context of the complete research life cycle from research agenda setting and call to proposal development, through grant application, allocation and management of funding, data production, analysis, management and sharing, to outputs, translation, and evaluation.”
Another conference speaker, Francis Kombe PhD, told attendees the statement will offer guidance specifically to institutions such as universities, journals, and funding organizations, the journal Science reported. That stands in contrast to earlier statements on helicopter research, which were geared more toward individuals and small groups.
How any of this will impact clinical laboratories and pathology groups remains unclear. Nevertheless, it is worthwhile knowing how gene sequencing is being used by researchers for purposes other than to guide diagnoses and treatment of patients.
DNA analysis of early plague victims pinpoints Black Death’s start on Silk Road trading communities in mountain region of what is now modern-day Kyrgyzstan in Central Asia
Microbiologists and clinical laboratory scientists will likely find it fascinating that an international team of scientists may have solved one of history’s greatest mysteries—the origin of the bubonic plague that ravaged Afro-Eurasia in the mid fourteenth century. Also known as the Black Death, the plague killed 60% of the population of Europe, Asia, and North Africa between 1346-1353 and, until now, the original source of this disease has largely gone unsolved.
In their study published in the journal Nature, titled, “The Source of the Black Death in Fourteenth-Century Central Eurasia,” the authors outlined their investigation of cemeteries in the Chüy Valley of modern-day Kyrgyzstan. The tombstone inscriptions showed a disproportionally high number of burials dating between 1338 and 1339 with inscriptions stating “pestilence” as the cause of death.
Archeological evidence combined with ancient DNA analysis of early plague victims enabled scientists to pinpoint the Black Death’s origins in Kyrgyzstan. “We have basically located the origin in time and space, which is really remarkable,” geneticist Johannes Krause, PhD (above), Professor at the Max Planck Institute for Evolutionary Anthropology, who co-led the study, told The Guardian. “We found not only the ancestor of the Black Death, but the ancestor of the majority of the plague strains that are circulating in the world today.” These new research findings may help microbiologists and clinical pathologists gain new insights into how current strains of Yersinia pestis can be better diagnosed. (Photo copyright: Max Planck Institute.)
Big Bang of Plague
Using 30 skeletons that were excavated from these cemeteries in the late 1880s and moved to St. Petersburg, Russia, the scientists analyzed the DNA of ancient pathogens recovered from the remains of seven people. They discovered Yersinia pestis (Y. pestis) DNA in three burials from Kara-Djigach, which lies in the foothills of the Tian Shan mountains.
According to another article in Nature, the scientists showed that a pair of full Y. pestis genomes from their data were direct ancestors of strains linked to the Black Death, and that the Kara-Djigach strain was an ancestor of the vast majority of Y. pestis lineages circulating today.
“It was like a big bang of plague,” Krause stated at a press briefing, Nature reported.
The research team concluded that the Tian Shan region was the location where Y. pestis first spread from rodents to people, and that the local marmot colonies likely the prevalent rodent carriers of plague.
“We found that modern strains [of the plague] most closely related to the ancient strain are today found in plague reservoirs around the Tian Shan mountains, so very close to where the ancient strain was found. This points to an origin of Black Death’s ancestor in Central Asia,” Krause explained in a Max Planck Institute news release.
He told Nature that fleas likely passed the marmot-based infection on to humans, sparking a local Kyrgyzstan epidemic. The disease then spread along the Silk Road trade routes, eventually reaching Europe, where rats (and the fleas that they carried) spread the disease.
Understanding Context of Plague
Writing in The Conversation, Associate Professor of Medieval and Environmental History Philip Slavin, PhD, University of Stirling, who co-authored the study, explained that Kara-Djigach is unlikely to be “the specific source of the pandemic,” but rather that the “disaster started somewhere in the wider Tian Shan area, perhaps not too far from that site,” where marmot colonies were likely the source of the 1338-1339 outbreak.
Making a modern-day comparison, Krause told Nature, “It is like finding the place where all the strains come together, like with coronavirus where we have Alpha, Delta, Omicron all coming from this strain in Wuhan.”
Slavin maintains that understanding the “big evolutionary picture” is key when studying the phenomenon of emerging epidemic diseases.
“It is important to see how these diseases develop evolutionary and historically, and avoid treating different strains as isolated phenomena,” he wrote in The Conversation. “To understand how the diseases develop and get transmitted, it is also crucial to consider the environmental and socioeconomic contexts.”
Scientists have spent centuries debating the source of the Black Death that devastated the medieval world. The multidisciplinary process used by the Slavin/Krause-led team provides a lesson to clinical laboratory managers and pathologists on the important role they play when collaborating with colleagues from different fields on scientific investigations.
Potentially increasing the revenue write-off burden for clinical laboratories, HRSA changes, insurance contracting, policy and coverage questions for genetic and genomic testing, and patient relationship disconnects will expose cracks in lab test claim generation and billing processes
Last year it was estimated that collection agencies held $140 billion in unpaid medical bills, in addition to the amount of unpaid bills in pre-collection status, according to a New York Times report. More recently, the American Hospital Association showed that hospitals have provided upwards of $700 billion in uncompensated care since 2000, with over $40 billion in 2019 alone.
Because strategies to collect the unpaid can be complicated and time-consuming, many healthcare organizations, including clinical laboratories, choose to write off these uncollectible bills. Dark Daily and The Dark Report have covered clinical laboratory revenue challenges for many years. In considering the paths forward, software-as-a-service (SaaS) provider FrontRunner Healthcare (FrontRunnerHC) recently provided snapshots into the how and where of improved collections.
Fixing Data Issues that Lead to Forfeited Clinical Laboratory Revenue
The underpinnings of unpaid lab tests are many. In a recent interview with Dark Daily, FrontRunnerHC CEO and Founder John (JD) Donnelly estimated that about one-third of claims (prior to submission) include incorrect or missing patient information, such as insurance policy identification or demographics. These gaps undermine an organization’s ability to get paid. Donnelly estimates that bad-debt write-offs for commercial payer claims average over 15% of charges. To address these challenges, the company’s clean claims SaaS provides “instantaneous” patient insurance, demographic, and financial information.
Whether lower-dollar accessions such as routine testing, or the higher-dollar accessions of genetic tests, uncollected payments add up. Donnelly said that, in 2021, almost one-third of the company’s clients uncovered revenue ranging from $1 million to over $90 million using the software. Donnelly also estimated that the return for clients averages eight times the value of the investment in using the automated solution.
In one example, Sonora Quest, a joint venture between Banner Health and Quest Diagnostics, reported a 10-15% decline in write-offs due to aged claims, a savings of over $1million annually, as published in a case study. “As an aside, in a presentation at the Executive War College last November, they also attributed improvements in patient satisfaction measures to the software, including a 65% decrease in abandoned calls, 28% improvement in their call service factor, and 19% decrease in patient call volumes,” stated Donnelly.
Questions About Cost of Care Likely Cause Stress for Patients
As many know, nonpay issues are problematic not only for lab businesses and anatomic pathology practices but also for patients and their families who have little predictability with their cost of care in the midst of stressful health events. “From the time a patient is registered to the time the claim is paid, there are more challenges than people realize that jeopardize the patient’s experience as well as the provider’s ability to get reimbursed,” Donnelly explained. Medical laboratory administrators have struggled to respond, often by using traditional manual methods such as call centers, or more recently by considering the use of data automation tools.
From the patient payment perspective, Donnelly said, a good strategy is having the ability, on demand, to understand each patient’s specific financial situation and likelihood to pay. For example, using FrontRunnerHC’s software to gauge patients’ propensity to pay and determine financial disposition strategies, lab administrators may choose to offer payment plans or hardship discounts to those falling under the federal poverty level (FPL). Or they may choose to send a collection agency only the past-due accounts for patients who have a low likelihood to pay rather than sending them all past due accounts and focus in-house efforts on the others. One genetics lab client who recently started leveraging these software capabilities “is already seeing more than 5% in incremental net collections,” according to Donnelly.
Further, an estimated 2 million people switch insurance plans each month, reported Axios. “That velocity of change is tough for providers to manage, but it’s critical as insurance eligibility and registration issues are the number one reason for claims denials,” Donnelly said.
For a sense of the magnitude of the problem, “Between 25 and 33 cents of every dollar you spend on medical care pays for health care’s back office,” wrote Dana Miller Ervin in September 2021 for a series of investigations called “The Price We Pay,” published at WFAE 90.7 news in Charlotte, North Carolina. “Every medical provider and laboratory in the country has to negotiate with insurance companies. And since there are 900 health insurers, 6,000 hospitals and more than 100,000 physician practices—many of which are independent of larger systems—there are hundreds of thousands of negotiations.”
New Clinical Laboratory Business Challenges Making News Now
All these issues affecting revenue cycle management (RCM) for independent clinical laboratories, hospital and health system laboratories, and physician office laboratories could be compounded by three emerging issues.
Donnelly said that many lab clients have yet to be reimbursed for COVID tests they have performed, despite their HRSA-required due diligence prior to submitting the claims before the deadline. To avoid additional reimbursement risk, many labs have made the decision to stop testing the uninsured or charge them for it, ABC News reported in late March. As of early April, however, Congress was in discussions to re-fund at least some of the Uninsured Program, reported Politico.
Secondly, and also daunting, are the questions surrounding payer coverage and reimbursement for genetic tests and genomic testing. Thanks to high-deductible health plans (HDHPs), clinical laboratories and anatomic pathology groups increasingly must collect deductibles that may be the full amount of the test – and directly from patients rather than from insurance companies. Therefore, there is more demand from patients to understand their expected cost before the test, Donnelly added.
Problems can arise, for both labs and patients, if they don’t know whether a test has been preauthorized for medical necessity or if they lack accurate insurance information such as in-network or out-of-network. “Getting all the needed and accurate info upfront prior to it going into the LIS [Laboratory Information System] can be a reimbursement game changer,” stated Donnelly.
“For a high complexity, high-throughput diagnostic lab, an efficient workflow is critical,” stated Kyle Koeppler, President of nuCARE Medical Solutions Inc., a FrontRunnerHC client. “Capturing the correct patient demographics and insurance information at patient intake increases the accuracy of every order and makes every process involving patient information much more efficient,” Koeppler shared. “It’s simply too costly to risk having inaccurate information at intake.”
And lest we forget, the Protecting Access to Medicare Act (PAMA) is looming with its reimbursement cuts planned through 2026, and requirements of many labs to report private payer rates on a test-by-test basis. While delayed again, the 2023 PAMA reporting requirements and payment cuts must not be ignored, and planning is needed in order to ensure appropriate reimbursement, Donnelly added.
Addressing Long Payment Cycles for Claims, Dead Ends, and Decreased Collection Rates
The CAQH report cites that data automation resulted in efficiency savings of $122 billion annually for the US healthcare system in 2020 yet “meaningful opportunities for additional savings remain.”
Data automation can reduce the burden of labor-intensive functions in coding, billing, filing appeals, and collecting from payers and patients and, therefore, reduce overall RCM costs. The Council for Affordable Quality Healthcare’s (CAQH) 2020 Index reported, “Considering the millions of times these transactions occur every day, the savings potential across the healthcare economy [from streamlining administrative processes] is significant.”
“One way to avoid potential write-offs is by reworking a claim, but the rework is often left undone,” stated John (JD) Donnelly (above), CEO and Founder of FrontRunnerHC. “The better way to avoid a potential write-off is to ensure you’ve got a clean claim in the first place.” (Photo copyright: FrontRunnerHC.)
The intended outcome is an increase in the total amount of revenue collected from the same number of claims.
To that end, FrontRunnerHC’s software links critical data within its partner ecosystem. This ecosystem includes the well-established credit reporting agencies as well as data available through connected healthcare payers and providers equipped with electronic data interchange (EDI) capabilities. “While an employee may be able to manually work about six accessions in an hour, clients can process approximately 40,000 patients in an hour through software automation, leaving staff to work on more value-added initiatives,” stated Donnelly.
Ideally, missing and inaccurate patient information or insurance verification, which are crucial for producing prompt payments and clean claims, should be corrected before a specimen is collected, Donnelly said. However, if the laboratory is nursing aging accounts receivable (AR), Donnelly advises an audit and cleanup of the AR backlog as a first step to quickly fix information errors and reduce write-offs. “In your AR bucket of $10 million, you may have $3 million that’s collectible or $9.8 million that’s collectible. By leveraging software to clean up what can be collected, clients can go after the money they deserve.”
Improve Collections Through Data Automation While Assisting in the Patient Financial Journey
With the rise of telehealth/telemedicine, healthcare consumerism, and care delivered to nontraditional sites, it makes sense that the idea of the clinical laboratory as a silent partner in healthcare could be changing.
“Could we one day see patients asked for not only their preferred pharmacy but their preferred clinical laboratory as well?” Donnelly pondered and added, “I think the answer is yes, and it’s sooner than many think.”
Understanding the patient’s experience is a key step in providing patient-centered care. Therefore, patient experience programs that originate at clinical laboratories where specimens are processed, but before specimens have been collected, could make these labs more visible in their markets and enable them to capitalize on the advantages of data automation to sustainably improve revenue cycle management.
“The patient’s financial journey which runs in parallel to their clinical journey can get pretty bumpy, and those bumps impact their overall experience as well as the provider’s bottom line,” added Donnelly. “Getting accurate patient information upfront and catching any changes to the information as needed throughout the process helps clients create a smoother patient journey by enabling them to quickly manage through the bumps or eliminate them altogether.”
—Liz Carey
This article was produced in collaboration with FrontRunnerHC.
Speakers at this week’s Executive War College in San Antonio explained that the way records are collected and stored plays a large part in the long-term usefulness of clinical laboratory data
Data structure as a term may not flow off the lips of clinical laboratory and pathology laboratory managers, but it should be top-of-mind. Well-structured data improves reimbursements and, in aggregated form, can be an enticing avenue to partnerships with outside parties.
Data structure refers to the makeup of digital records—in other words, how data is collected, stored, and accessed. Structured information offers consistency and is easier to analyze and share.
“You have to make sense of all that messy data, and that’s a heavy lift,” she said. “Results are not standardized.”
Appeals Payments Increase with More Clinical Data
Data quality can improve claim reimbursement appeals, Goede noted. When a more complete clinical record is provided to payors, they are more likely to reimburse for services.
According to information Goede covered along with Julie Ramage, Director of Precision Medicine Quality Initiatives and Partnerships at biopharmaceutical company AstraZeneca, when appealing a denied claim for a colon cancer molecular test, for example, the average appeal payment was $318 without cross-specialist clinical records.
Meanwhile, payment for a similar claim appeal which included that added data jumped to $612!
This information is often available, but may not be structured in a way that makes it easy to share with a payer. “You really have to be thinking about what elements you need,” Goede said.
Market for Structured, Anonymized Lab Data
Clinical laboratories that want to provide or sell anonymized, aggregated data to outside parties—such as research firms or pharmaceutical companies—also need to pursue efficient data structure. The re-use of existing, high-quality lab data can create a new business revenue stream.
“But it has to be more than that vanilla, male/female, date-of-birth stuff,” Ramage noted.
For example, she said, genetic testing builds up data registries, and that’s what pharma is looking for to find patients early on.
“If you don’t have a way to structure your data, you’re not going to be able to play in the sandbox,” she added.
Co-presenters Julie Ramage (left), Director of Precision Medicine Quality Initiatives and Partnerships at AstraZeneca Pharmaceuticals, and Patricia Goede, PhD (right), Vice President of Clinical Informatics at XIFIN, Inc., answer attendee questions about data structure during their presentation at this week’s Executive War College Conference on Laboratory and Pathology Management in San Antonio. To register for EWC 2022 and receive a special early-bird rate, click here by November 6.
How Clinical Laboratories Can Improve Clinical Data Structure
Here are some tips for clinical laboratory executives to consider as they tackle data structure:
Standardize how to enter patient information and test results. A common problem with data input is that the same information is entered differently over time. For example, various patient records might refer to dates in different ways: November 1, 2021, can also be entered as 11/1/21, 11/1/2021, or 11-01-21. Structured data uses a single way to list dates in records. This lesson applies to all similar clinical data.
Use dropdown menu choices instead of free-typing, open fields. An online box to enter a test result can create a variety of entries that affect data structure. While not perfect, drop-down options create a consistent set of entries, Goede said.
Ask patient advocacy groups about common nomenclature. Clinical laboratory data should reflect how patients speak, Ramage said. For example, do patients refer to genomic and genetic testing as the same thing? Establishing more consistency improves data structure as records are updated.
Enlist your organization’s IT or research team for help. Tech workers and principal investigators can easily look at clinical laboratory data and tell what information is missing or inconsistent, said Cheryl Schleicher, Director of IT Strategy at Northwell Health Labs in Lake Success, NY. Schleicher attended this week’s Executive War College.
Look Further into Clinical Laboratory Data Structure
Data structure can help clinical laboratories and pathology laboratories grab more reimbursement dollars and potentially sell anonymized data to external partners.
It is an area many lab executives are not familiar with and need to investigate more, particularly following the accelerated move to digital lab services during the COVID-19 pandemic. Your organization’s IT department or Chief Information Officer can be a useful ally.
If you could not make it to this week’s Executive War College, then join us for our next Executive War College on April 27-28, 2022, in New Orleans. Click here to take advantage of special early-bird pricing for this critical event.
It did not take long for fraudsters to pursue hundreds of billions of federal dollars designated to support SARS-CoV-2 testing and it is rare when federal prosecutors bring cases only a few months after illegal lab testing schemes are identified
As if the COVID-19 pandemic weren’t bad enough, unscrupulous clinical laboratory operators quickly sought to take advantage of the critical demand for SARS-CoV-2 testing and defraud the federal government.
Unfortunately for the many defendants in these cases, federal investigations into alleged cases of fraud were launched with noteworthy speed. As a result of these investigations into alleged healthcare fraud by clinical laboratories and other organizations during fiscal year (FY) 2020, the US Department of Justice (DOJ) announced the US government has recovered $1.8 billion.
The federal prosecutions involved dozens of medical laboratory owners and operators who paid back “hundreds of millions in alleged federal healthcare program losses,” Goodwin Life Sciences Perspectives explained.
When combined with similar efforts starting in prior years, the program has returned to the federal government and private individuals a total of $3.1 billion, the DOJ noted.
“In its 24th year of operation, the program’s continued success confirms the soundness of a collaborative approach to identify and prosecute the most egregious instances of healthcare fraud, to prevent future fraud and abuse, and to protect program beneficiaries,” the report states.
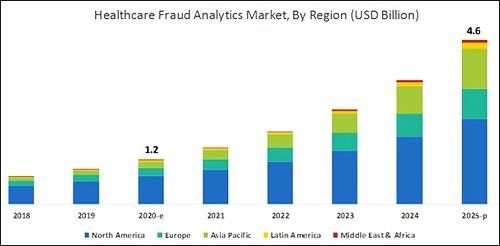
According to the graphic above, which is based on analysis by B2B research company MarketsandMarkets, “North America will dominate the healthcare fraud analytics market from 2020–2025.” As clinical laboratory testing represents a significant portion of the fraud, medical lab managers will want to remain vigilant. (Graphic copyright: MarketsandMarkets.)
COVID-19 Pandemic an Opportunity for Fraud
The HHS report notes that the COVID-19 pandemic required CMS to develop a “robust fraud risk assessment process” to identify clinical laboratory fraud schemes, such as offering COVID-19 tests in exchange for personal details and Medicare information.
“In one fraud scheme, some labs are targeting retirement communities claiming to offer COVID-19 tests but are drawing blood and billing federal healthcare programs for medically unnecessary services,” the HHS report notes.
Still other alleged schemes involved billing for expensive tests and services in addition to COVID-19 testing. “For example, providers are billing a COVID-19 test with other far more expensive tests such as the Respiratory Pathogen Panel (RPP) and antibiotic resistance tests,” the report says.
“Other potentially unnecessary tests being billed along with a COVID-19 test include genetic testing and cardiac panels CPT (current procedural terminology) codes. Providers are also billing respiratory, gastrointestinal, genitourinary, and dermatologic pathogen code sets with the not otherwise specified code CPT 87798,” the report states.
Different Types of Healthcare Organizations Investigated in 2020
Beyond clinical laboratories, the HHS’ 124-page report also shares criminal and civil investigations of other healthcare organizations and areas including:
clinics,
drug companies,
durable medical equipment,
electronic health records,
home health providers,
hospice care,
hospitals and healthcare systems,
medical devices,
nursing home and facilities,
pharmacies, and
physicians/other practitioners.
According to the DOJ, “enforcement actions” in 2020 included:
1,148 new criminal healthcare fraud investigations opened,
440 defendants convicted of healthcare fraud and related crimes,
1,079 civil healthcare fraud investigations opened, and
1,498 pending civil health fraud matters at year-end.
“Federal Bureau of Investigation (FBI) investigative efforts resulted in over 407 operational disruptions of criminal fraud organizations and the dismantlement of the criminal hierarchy of more than 101 healthcare fraud criminal enterprises,” the DOJ reported.
Furthermore, the report said OIG investigations in 2020 led to:
578 criminal actions against people or organizations for Medicare-related crimes,
781 civil actions such as false claims, and
2,148 people and organizations eliminated from Medicare and Medicaid participation.
Implications for Clinical Laboratories
In 2020, OIG issued 178 reports, completed 44 evaluations, and made 689 recommendations to HHS divisions.
Clinical laboratory leaders may be most interested in those related to patient identification as a means to combating fraud and Medicare Part B lab testing reimbursement.
The HHS report says, “Medicare Advantage (MA) encounter data continue to lack National Provider Identifiers (NPIs) for providers who order and/or refer … clinical laboratory services,” adding that, “Almost half of MA organizations believe that using NPIs for ordering providers is critical for combating fraud.”
Additionally, the report states, “Medicare Part B spending for lab tests increased to $7.6 billion in 2018, despite lower payment rates for most lab tests. The $459 million spending increase was driven by:
“increased spending on genetic tests,
“ending the discount for certain chemistry tests, and the
“move to a single national fee schedule.”
Medical laboratory leaders may be surprised to learn that federal healthcare investigators were so vigorous in their investigations, even during the worst of the COVID-19 pandemic.
Vigilance is critical to ensure labs do not fall under the DOJ’s scrutiny. This HHS report, which describes the types and dollars involved in fraudulent schemes by clinical labs and other providers, could help inform revisions to federal compliance regulations and statutes.