Clinical laboratory scientists should also know experts warn that ‘herd resistance’ is more likely than ‘herd immunity’ due to low vaccination rates in many parts of the world
Scientists estimate 73% of the US population may be immune to the SARS-CoV-2 omicron variant. Whether the nation is approaching “herd immunity” against the disease, however, remains open to debate, the Associated Press (AP) reported. These estimates are relevant to medical laboratories doing serology tests for COVID-19, as different individuals will have different immune system responses to COVID-19 infections and vaccines.
More than two years into the COVID-19 pandemic in the United States, the CDC’s COVID Data Tracker shows the number of daily cases dropped to fewer than 50,000 as of March 4, 2022, after reaching a high of 928,125 on January 3, 2022.
Meanwhile, the seven-day death rate per 100,000 people stands at 2.78. That’s significantly above the seven-day death rate reached last July of .45, but well below the 7.21 mark recorded on January 13, 2021.
“We’re clearly entering a new phase of the pandemic,” William Morice, II, MD, PhD, Department of Laboratory Medicine and Pathology at Mayo Clinic in Rochester, Minn., told KARE11, an NBC affiliate.
Is Herd Immunity Achievable?
According to the AP, an estimated 73% of the US population is likely to be immune to the Omicron variant due to vaccination or natural immunity from contracting the disease. That calculation was done for the media outlet by the Institute for Health Metrics and Evaluation (IHME) at the University of Washington in Seattle. The IHME anticipates immunity to Omicron could rise to 80% this month, as more people receive vaccination booster shots or become vaccinated.
“Herd immunity is an elusive concept and doesn’t apply to coronavirus,” he told the Associated Press (AP).
Milton maintains populations are moving toward “herd resistance,” rather than “herd immunity.” This will transform COVID-19 into a permanent fixture with seasonal outbreaks similar to influenza.
Epidemiologist, Ali Mokdad, PhD (above), Chief Strategy Officer for Population Health and Professor of Health Metrics Science at the University of Washington in Seattle, believes the US is now much better positioned to withstand the next wave of COVID-19 cases. “I am optimistic even if we have a surge in summer, cases will go up, but hospitalizations and deaths will not,” he told the Associated Press (AP). Mokdad worked on the IHME model that calculated the 73% Omicron-immunity figure for the AP. However, he recommends continued vigilance toward COVID-19. “We’ve reached a much better position for the coming months, but with waning immunity we shouldn’t take it for granted,” he added. And so, clinical laboratories can expect to continue to play a vital role in the fight against the spread of the SARS-CoV-2 coronavirus. (Photo copyright: University of Washington.)
Herd Immunity Varies, according to the WHO
Because antibodies that developed from vaccines—or natural immunity from a previous infection—diminish over time, waning protection means even those boosted or recently recovered from COVID-19 could be reinfected. In addition, vaccination rates vary widely around the world. Our World in Data estimates only 13.6% of people in low-income countries had received one dose of the COVID-19 vaccine as of March 7, 2022.
The World Health Organization (WHO) points out that herd immunity levels vary with different diseases. Herd immunity against measles requires about 95% of a population to be vaccinated, while the threshold for polio is about 80%.
“The proportion of the population that must be vaccinated against COVID-19 to begin inducing herd immunity is not known. This is an important area of research and will likely vary according to the community, the vaccine, the populations prioritized for vaccination, and other factors,” the WHO website states.
Living with COVID-19
Nonetheless, the US appears to be moving into a new “normal” phase of living with the disease.
In an interview with Reuters, US infectious disease expert Anthony Fauci, MD, Director of the National Institute of Allergy and Infectious Diseases (NIAID) acknowledged a need for returning to normal living even though portions of the population—immunocompromised individuals and the unvaccinated, including children under age five who are not eligible for vaccination—remain vulnerable to more severe COVID-19.
“The fact that the world and the United States—and particularly certain parts of the United States—are just up to here with COVID, they just really need to somehow get their life back,” Fauci said. “You don’t want to be reckless and throw everything aside, but you’ve got to start inching towards that. There’s no perfect solution to this.”
Most states have lifted coronavirus-related restrictions, including masking requirements. As COVID-19 cases drop in California, Gov. Gavin Newsom put in motion a plan called SMARTER (Shots, Masks, Awareness, Readiness, Testing, Education, and Rx) that no longer responds to COVID-19 as a crisis, but instead emphasizes prevention, surveillance, and rapid response to future variant-based surges in cases.
“We have all come to understand what was not understood at the beginning of this crisis, that there’s no ending, that there’s not a moment where we declare victory,” Newsom told USA Today.
Mayo Clinic’s Morice agrees. “It can’t be out of sight, out of mind, per se, but it at least gives us hope that we can get back to some level of normalcy here over the course of the year,” he said.
Since clinical laboratories played a critical role in assay development and COVID-19 testing, medical laboratory leaders should continue monitoring COVID-19 as it moves from pandemic to endemic status due to high vaccination rates and advances in treatment options.
The COVID-19 pandemic has raised awareness among healthcare consumers as well, about the critical role laboratory medicine plays in modern medicine and healthcare. Medical laboratory leaders and pathologists would be wise to amplify this message and stress the importance of clinical laboratory testing for many diseases and healthcare conditions.
According to the Centers for Disease Control and Prevention (CDC), the 1918 influenza (aka, the Spanish Flu) pandemic took place worldwide between 1918 and 1919. It was caused by the H1N1 virus (A/H1N1), a subtype of the Influenza A virus, and infected approximately 500 million people worldwide (a third of the human population at the time). Fifty million people died. Many were children or otherwise healthy individuals, but people from all age groups perished.
The CDC calls the Spanish Flu the “deadliest pandemic of the 20th century.” Past pandemics have generally concluded after 2.5 to 3.5 years. That’s how long it takes for new viruses to mutate and become endemic diseases, Healthline reported.
The COVID-19 pandemic has been around for about that long. It stands to reason the natural end of the COVID-19 pandemic may be just around the corner. But is it? And is the Omicron variant an indicator that the COVID-19 pandemic is winding down?
“Our analysis suggests that in the US, this combination of characteristics would lead to Omicron replacing Delta as the dominant variant in the next few months and to a higher peak burden of disease than the country saw in the second half of 2021 (but likely below the peak reached in the winter of 2020-21),” the report states.
McKinsey analysts also acknowledged the possible impact of new therapeutics, COVID-19 vaccine booster doses, and public health measures on Omicron spread. “In the short term, an accelerated rollout of booster doses of COVID-19 vaccines is likely to be one of the best protections against an Omicron-fueled wave of the disease,” the analysts wrote.
Does How the Spanish Flu Came to an End Mirror the COVID-19 Pandemic?
Virologists and infectious disease experts explained that the Spanish Flu virus did what viruses still do: mutate and become less dangerous. Herd immunity also helped end the 1918 pandemic.
“The 1918 influenza virus eventually mutated to the point of not having a high number of deaths—eventually over three years or so. We may very well be witnessing this process with ongoing variants of SARS-CoV-2,” virologist Rodney Rohde, PhD, Director of the Clinical Laboratory Science Program at Texas State University, told Healthline.
Today’s flu strains have “ancestral links” to the 1918 flu, and thus, the SARS-CoV-2 coronavirus will most likely also leave its mark, The Boston Herald reported. “The coronavirus will evolve and hopefully morph into a seasonal illness to which we pay little mind, but it’s still too early to tell,” Todd Ellerin, MD (above,) Director of Infectious Diseases, South Shore Health, South Weymouth, Mass., told The Boston Herald. (Photo copyright: Greg Derr/The Patriot Ledger.)
“If you think about the way viruses behave, biologically, their reason for living is to replicate and spread, and there’s really no advantage for the virus to kill the host,” infectious disease specialist Keith Armitage, MD, Professor of Medicine, Division of Infectious Diseases at Case Western Reserve University, told Healthline. “The hope is, that if the pandemic doesn’t go away, we will get new variants that are highly contagious but don’t produce much of a clinical illness,” he added.
In “2021’s Top 10 Lab Stories Confirm Important Trends,” Dark Daily’s sister publication, The Dark Report (TDR), posed a similar question in its number one story of 2021: “COVID-19: Will it Become Endemic and a Respiratory Virus that Shows Up Every Year like Influenza?”
“The question of whether SARS-CoV-2 is a pandemic that fades, as did SARS in 2003, or becomes endemic and a respiratory virus that shows up every season like influenza and the common cold, is of major concern to clinical lab administrators. That’s because clinical labs and pathology groups must continue to serve physicians and patients with the usual menu of routine, reference, and esoteric testing,” TDR noted.
Clinical Laboratories to Continue COVID Testing
It would be most helpful for medical laboratories and pathology groups to have some idea of when the pandemic will end. Unfortunately, such predictions would not be very useful.
“Since COVID-19 infections have a high number of asymptomatic transmitters, we may not fully understand how societal and environmental pressures—masks, distancing, remote working, etc.—on the virus will allow it to evolve,” Rohde told Healthline.
For now, clinical laboratories will need to continue to remain prepared as COVID-19 cases rise and people seek SARS-COV-2 tests, vaccinations, and treatments. COVID-19 testing is likely to be in demand throughout the coming year. The current surge in demand for COVID-19 tests is putting additional stress on the supply chain.
“We know pandemics end; it’s just a matter of time,” Sara Paton, PhD, Associate Professor of Epidemiology, Wright State University, told the Journal-News. “It could be in 2022, maybe later in the year, but I can’t say for sure. It could be 2023.”
The latest McKinsey report addresses when the COVID-19 pandemic is “most likely” to end and what needs to happen to get there
Clinical laboratory leaders, pathologists, and diagnostics professionals everywhere want to know when the SARS-CoV-2 coronavirus will burn itself out. When can we expect to return to normal? Since there is no such thing as a crystal ball, it might be helpful to review the latest report from international management consulting firm McKinsey and Company, titled, appropriately, “When Will the COVID-19 Pandemic End?”
It’s a good question, and McKinsey is not certain of the answer. Barring other factors, McKinsey predicts “Transition toward normalcy in the United States remains most likely in the second quarter of 2021 and herd immunity in the third and fourth quarters, but the emergence of new strains and a slow start to vaccine rollout raise real risks to both timelines.” The report also states, “the emergence of more-infectious variants of SARS-CoV-2 increases the risk that this milestone will not be achieved until later.
“More-infectious viruses,” McKinsey continued, “require that a higher percentage of people be simultaneously immune to reach herd immunity. While a more infectious variant likely means more people are acquiring natural immunity through infection (despite ongoing efforts to minimize new cases), the net impact of more-infectious strains is likely to be that a higher portion of the population needs to be vaccinated, which may take more time.”
Challenges That May Slow Herd Immunity to COVID-19
“It is now harder to imagine the United States or United Kingdom transitioning to normalcy before second quarter 2021 or reaching herd immunity before third quarter 2021,” McKinsey added. “Herd immunity to a pathogen is achieved when a sufficient portion of a population is simultaneously immune to prevent sustained transmission.”
But problems in [COVID-19] vaccine distribution, supply shortages, and intermittent participation by the population could push the pandemic endpoint to 2022, cautioned McKinsey.
“We believe herd immunity in the United States is still most likely in third or fourth quarter 2021, but that the chance of delay until first quarter 2022 or beyond has increased,” the report states, “Even later herd immunity remains possible if other challenges arise, especially vaccine safety concerns or ambivalence to vaccination following a transition toward normalcy.”
Other factors that went into the firm’s “most likely” set of possible timelines include:
“Unexpected safety issues emerging with early vaccines,
“Significant manufacturing or supply-chain delays,
“Continued slow adoption,
“Further mutation [of the virus],
“A shorter-than-anticipated duration of vaccine-conferred immunity.”
The graph above, taken from the McKinsey and Co. report, illustrates how “the probability of reaching COVID-19 herd immunity in the United States is highest in the third or fourth quarter, but could shift.” (Graphic copyright: McKinsey and Company.)
A ‘Transition Toward Normalcy’
In its report, McKinsey notes that “During this transition, controlling the spread of SARS-CoV-2 will still require public-health measures (such as continued COVID-19 testing and mask use in many settings), but mortality will fall significantly, allowing greater normalization of business and social activities.”
In apparent agreement, according to data from the COVID Tracking Project, as of Jan. 27, 2021, 107,444 people were hospitalized in the US with COVID-19, as compared to 130,000 hospital cases on Jan. 13, 2021. Numbers of new cases appear to be dropping, however, McKinsey predicts that “COVID-19 will not disappear during this transition but will become a more normal part of the baseline disease burden in society (like flu, for example), rather than a special threat requiring exceptional societal response.”
It may help that more people are taking one of the vaccines. A recent survey conducted by London-based research and analytics firm YouGov, found that people worldwide are becoming more willing to take the COVID-19 vaccine. For example, in the UK, 80% of those surveyed gave a thumbs-up to getting vaccinated, compared to 61% in November. In the US, however, still only about 45% said they will get the vaccine, up slightly from 42% who said so in July, YouGov reported.
However, McKinsey points out that “vaccine rollout has not yet proceeded far enough to protect much of the population.”
How Should Medical Laboratories and Other Healthcare Providers Proceed?
In “No One Said it Would Be Easy,” Jan. 22, 2021, Becker’s Hospital Review, Michael Dowling, President and CEO of Northwell Health, wrote, “We will be living in a world preoccupied by COVID-19 and vaccination for many months to come … And the stark reality is that the vaccination rollout will continue well into the summer, if not longer, while at the same time we continue to care for hundreds of thousands of Americans sickened by the virus. Despite the challenges we face now and in the coming months in treating the disease and vaccinating a US population of 330 million, none of us should doubt that we will prevail.”
“To achieve that,” McKinsey notes, “we will need to see significant progress on the epidemiological end point … Favorable findings on natural and cross-immunity would help accelerate timelines.
“Five additional criteria will also contribute to the transition to a form of normalcy—the more of these that are achieved, the faster the milestone is likely to be reached:
“Continued improvement by governments in the application of public-health interventions (such as test and trace) that don’t significantly limit economic and social activities.
“Compliance with public-health measures until we achieve herd immunity.
“Accurate, widely available, rapid testing that effectively enables specific activities.
“Continued advancements in therapeutics (including pre- and post-exposure prophylactics) for and clinical management of COVID-19, leading to lower infection-fatality ratios—substantial progress has already been made through a combination of effective drugs, such as Dexamethasone and Remdesivir, and changes in clinical management.
“Public confidence that there aren’t significant long-term health consequences for those who recover from COVID-19.”
Finally, McKinsey notes that “Both the epidemiological and normalcy ends to the COVID-19 pandemic are important. The transition to the next normal will mark an important social and economic milestone, and herd immunity will be a more definitive end to the pandemic. In the United States, while the transition to normal might be accomplished sooner, the epidemiological end point looks most likely to be reached in the second half of 2021.”
It is not clear when clinical laboratories and pathologists will know for certain when the pandemic’s end point has been reached. Predictions coming from sources such as McKinsey’s latest report may be as close as we get to a crystal ball view of the pandemic’s future.
Researchers conducted antibody testing on ‘remainder plasma,’ which could inform strategies for ongoing SARS-CoV-2 clinical laboratory surveillance testing
In a clever use of stored clinical laboratory specimens, researchers in California conducted a nationwide seroprevalence survey—serology testing to determine the number of people in a population that carry a specific disease—that used “remainder plasma” from dialysis patients to look for antibodies to the COVID-19 infection. They found that—as of July—fewer than one in 10 adults tested had acquired antibodies to the SARS-CoV-2 coronavirus.
According to Julie Parsonnet, MD, Stanford Professor of Medicine and of Epidemiology and Population Health, and a study author, this indicates that the US population is a long way from herd immunity to COVID-19. “This is the largest study to date to confirm that we are nowhere near herd immunity,” she said in a Stanford Medicine press release.
Herd immunity is the point at which a large part of the population becomes immune to a specific disease. Scientists, according to the Stanford press release, estimate that 60%-70% of the population must have antibodies to the coronavirus before COVID-19 fades.
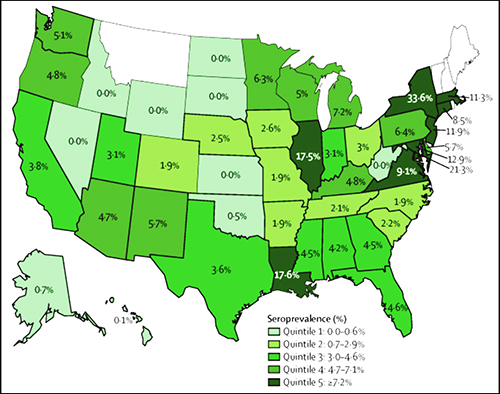
The graphic above taken from Stanford Medicine’s published study illustrates the “prevalence of SARS-CoV-2 antibodies in sampled population, by state. Bolded borders represent states with more than 100 patients in the sample. The median number of patients sampled by state was 176 (IQR 83–536). States in white were not sampled.” (Graphic copyright: Stanford University.)
Dense Urban Populations at Greater Risk for COVID-19
The Stanford researchers analyzed samples of remainder plasma from 28,503 randomly selected patients receiving dialysis in July at more than 1,300 dialysis facilities in 46 states. They found that 8% of people were positive for COVID-19 antibodies, which when standardized to the US adult population, equals 9.3% nationwide, the study notes.
However, they also found that people living in densely populated areas were 10 times more likely to show evidence of past COVID-19 infection, and that people living in predominantly black and Hispanic neighborhoods were two to three times more likely to be seropositive than those in white neighborhoods, the researchers wrote.
Of the use of remainder plasma for their study, the researchers wrote, “Testing remainder plasma from monthly samples obtained for routine care of patients on dialysis for SARS-CoV-2 antibodies therefore represents a practical approach to a population-representative surveillance strategy, informing risks faced by a susceptible population while ensuring representation from racial and ethnic minorities.
“In addition, seroprevalence surveys in patients receiving dialysis can be linked to patient-level and community-level data to enable evaluation and quantification of differences in SARS-CoV-2 prevalence by demographic and neighborhood strata, and thus facilitate effective mitigation strategies targeting the highest-risk individuals and communities,” added the researchers.
When standardized to the US dialysis population, seroprevalence ranged from 3.5% (95% CI, 3.1-3.9) in the West to 27.2% (95% CI, 25.9-28.5) in the Northeast.
Large variations in seroprevalence by state were seen, with early COVID-19 hot spots such as New York (33.6%), Louisiana (17.6%), and Illinois (17.5%) having higher rates than neighboring states—Pennsylvania (6.4%), Arkansas (1.9%), and Missouri (1.9%).
When compared with other measures of SARS-CoV-2 spread, seroprevalence correlated best with deaths per 100,000 population.
“With this survey, we were able to provide a very rich picture of the first wave of the COVID-19 outbreak in the U.S. that can hopefully help inform strategies to curb the epidemic moving forward by targeting vulnerable populations,” said Shuchi Anand, MD (above left, with fellow Nephrologists Colin Lenihan and Michelle O’Shaughnessy), Director of Stanford’s Center for Tubulointerstitial Kidney Disease and lead author of the study. (Photo copyright: Stanford Medicine.)
Nearly 10% of COVID-Positives Are Undiagnosed
In another important finding that compared seroprevalence and case counts per 100,000 population as of June 15, the study reports that only 9.2% of the COVID-19 seropositives had been diagnosed with the disease.
Because dialysis patients get monthly laboratory blood tests that generate leftover blood plasma samples, researchers believe this remainder plasma can serve an important role in tracking COVID-19’s prevalence in the general population.
“Not only is this patient population representative of the US population, but they are one of the few groups of people who can be repeatedly tested,” said Anand in the Stanford press release. “This is a potential strategy for ongoing SARS-CoV-2 antibody testing and surveillance.”
“Questions remain around the longevity of the immune response and correlates of protection, but high-quality longitudinal serosurveillance with accompanying clinical data can help to provide the answers,” they wrote. “Anand and colleagues deserve credit for pioneering a scalable sampling strategy that offers a blueprint for standardized national serosurveillance in the USA and other countries with a large haemodialysing population.”
Pandemic Fatigue and the Vaccine
While the promised vaccine provides hope for an end to the pandemic, experts say the battle is far from won.
“We are still in the middle of the fight,” epidemiologist Eli Rosenberg, PhD, Associate Professor at the University at Albany in New York, who was not part of the Stanford study, told the Washington Post, “We’re all tired, and we’re all hoping for a vaccine. This shows us how it’s not over here, not even by a long shot.”
What is obvious is that clinical laboratories will continue to play a vital role in response to the COVID-19 pandemic. In fact, just as the management and scientific team at Ascend Clinical Laboratories recognized that remainder plasma from testing dialysis patients could be the foundation of a national seroprevalence survey for COVID-19, other clinical laboratories in different regions of the United States may have similar resources that can be adapted as tools to study and understand the SARS-CoV-2 pandemic.