Clinical laboratories may see increase in flu and COVID-19 specimen processing as people return to pre-pandemic social behaviors, experts predict
While SARS-CoV-2 infections continue to ravage many parts of the world, influenza (flu) cases in North America have hit a historic low. As winter approached last year, infectious disease experts warned of a “twindemic” in which the COVID-19 outbreak would combine with seasonal influenza to overwhelm the healthcare system. But this did not happen, and many doctors and medical laboratory scientists are now investigating this unexpected, but welcomed, side-effect of the pandemic.
From the start of the current flu season in September 2020, clinical laboratories in the US reported that 1,766 specimens tested positive for flu out of 931,726—just 0.2%—according to the CDC’s Weekly US Influenza Surveillance Report. That compares with about 250,000 positive specimens out of 1.5 million tested in the 2019-2020 flu season, the CDC reported. Public health laboratories reported 243 positive specimens out of 438,098 tested.
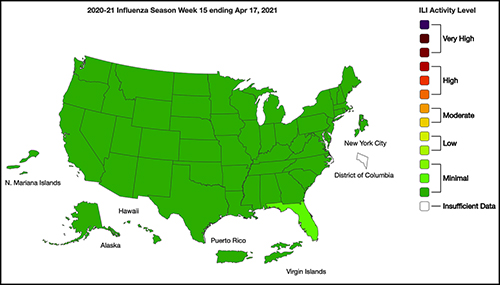
The graphic above taken from the CDC’s Weekly Influenza Surveillance Report for the week ending April 17, 2021, illustrates how “Nationwide during week 15, 1.1% of patient visits reported through ILINet were due to ILI [Influenza-like Illness].” This percentage, according to the CDC, is below the national baseline of 2.6%. “Seasonal influenza activity in the United States remains lower than usual for this time of year.” (Graphic copyright: Federal Centers for Disease Control and Prevention.)
Fear of COVID-19 Linked to Fewer Flu Deaths in Children
WebMD reported that just one child in the US has died from the flu this year, compared with 195 in 2020. Why the low numbers?
Precautions people take to avoid COVID-19 transmission, including masking, social distancing, and handwashing.
Reduced human mobility, including less international travel.
Higher-than-usual flu vaccination rates. As of February 26, the CDC reported that nearly 194 million doses of flu vaccine had been distributed in the US.
WebMD noted this could be a record, but that the CDC data doesn’t indicate how many doses were actually administered.
However, Schaffner told WebMD that efforts to keep kids home from school and away from social gatherings were likely a bigger factor. “Children are the great distributors of the influenza virus in our society,” he said. But due to fears about COVID-19 transmission, kids “weren’t even playing together, because mothers were keeping them off the playground and not having play dates.”
Repercussions for Fighting Flu Next Year
Public health experts welcomed the low flu levels, however, Politico reported that limited data about flu circulation this year could hamper efforts to develop an effective vaccine for next season’s flu strains.
Each February, Politico explained, experts convened by the World Health Organization (WHO) look at data from the current and previous flu seasons to predict which strains are likely to predominate in the Northern Hemisphere next winter. That includes data about which strains are currently circulating in the Southern Hemisphere. The WHO uses these predictions to recommend the composition of flu vaccines. In the US, the final decision is made by an FDA advisory committee.
A similar WHO meeting in September guides vaccine development in the Southern Hemisphere.
The WHO issued this year’s Northern Hemisphere recommendations on Feb. 26. The advisory includes recommendations for egg-based and cell- or recombinant-based vaccines, and for quadrivalent (four-strain) or trivalent (three-strain) vaccines.
In a document accompanying the recommendations, the WHO acknowledged concerns about this year’s limited pool of data.
“The volume of data available from recently circulating influenza viruses, and the geographic representation, have been significantly lower for this northern hemisphere vaccine recommendation meeting than is typical,” the document stated. “The reduced number of viruses available for characterization raises uncertainties regarding the full extent of the genetic and antigenic diversity of circulating influenza viruses and those likely to pose a threat in forthcoming seasons.”
The report notes that experts identified changes in circulating Influenza A(H3N2) viruses this year, and that the changes are reflected in the new vaccine recommendation.
But Paul A. Offit, MD, who serves on the FDA’s vaccine advisory panel, downplayed worries about the vaccine. “The belief is that there was enough circulating virus to be able to pick what is likely to be the strains that are associated with next year’s flu outbreak,” he told Politico. Offit is a Professor of Vaccinology and Pediatrics at the Perelman School of Medicine at the University of Pennsylvania and Director of the Vaccine Education Center at the Children’s Hospital of Philadelphia.
Pediatrician and internationally recognized expert in the fields of virology and immunology, Paul A. Offit, MD (above), told Politico that the low level of flu circulation this year, along with the resulting uncertainty, “is unprecedented.” Clinical laboratories might not have noticed the severe decrease in influenza specimens sent for processing due to being hyper-focused on COVID-19 testing. But as the pandemic subsides, loss of flu testing revenues will likely become more apparent. (Photo copyright: University of Pennsylvania.)
Offit suggests that efforts to mitigate the COVID-19 outbreak could be useful to combat other infectious disease outbreaks. However, both Offit and Gostin expressed doubt about that prospect.
“I mean, could we reasonably in a winter month, wear masks just at least when we’re outside in large crowds? … Or are we comfortable having hundreds of 1000s of cases of hospitalizations for flu and 10s of 1000s [of] deaths? I suspect the answer is B. We’re comfortable with that, we’re willing to have that even though we just learned, there’s a way to prevent it,” Offit told Politico.
“Remember after the 1918 flu pandemic, most people don’t realize what happened when that was over. But what happened was the roaring ‘20s,” Gostin told Politico. “People started congregating, mingling, hugging, kissing. All the things they missed. They crowded into theaters and stadiums and went back to church. That’s what’s likely to happen this fall and that makes the influenza virus very happy.”
So, what should clinical laboratories expect in future flu and COVID-19 vaccines? That is not yet clear. One thing is certain, though. New lab test panels that test for influenza and the SARS-CoV-2 coronavirus will be arriving in the marketplace.
The remarkably low number of influenza diagnoses makes it possible for clinical laboratories to stay focused on COVID-19
One positive note for clinical laboratories this winter is the fact that the number of biological samples being submitted for influenza (flu) testing have dropped significantly. This has given medical laboratories more resources for processing COVID-19 tests.
According to a feature published in Nature, the number of samples being submitted to medical laboratories for flu testing has dropped by 61%. More surprisingly, the number of positives has dropped by 98%. The combined flu/COVID-19 “twindemic” that some medical experts feared could crush our healthcare system has not materialized—yet, the Washington Examiner reported.
“In any given winter, hospitals are taxed by the flu,” Brian Garibaldi, MD, a pulmonologist and critical care specialist and Medical Director of the Johns Hopkins Biocontainment Unit told the Washington Examiner. “There’s always a concern that our emergency departments will be overwhelmed, and ICU capacity will be strained [due to the concurrence of flu and COVID-19 outbreaks], particularly with people who have coexisting conditions that then get influenza.”
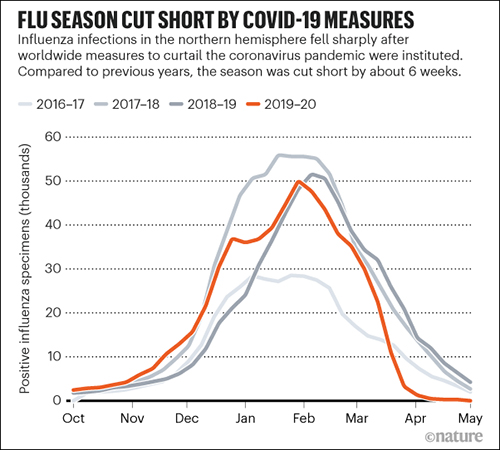
The 2019-2020 flu season ended earlier than usual, likely because of precautions put in place in the spring to combat the coronavirus pandemic. Most years, the seasonal flu in the US peaks in February and trails off by May, Nature reported in “How Coronavirus Lockdowns Stopped Flu in Its Tracks.”
“Seasonal flu cases in the northern hemisphere usually peak in February and tail off by the end of May,” Nature wrote. “This year, unusually, lab-confirmed cases of influenza dropped precipitously in early April, a few weeks after the coronavirus pandemic was declared on 11 March. The data comes from tests of more than 150,000 samples from national influenza laboratories in 71 countries that report data to FluNet, a global surveillance system.”
Government Leaders and Health Experts Remain Concerned
Despite that encouraging data point, public health experts and political leaders were still concerned. In September, Arizona Governor Doug Ducey said, “The overlap of COVID-19 and flu season presents a perfect storm, and we aren’t taking any chances. We are approaching this fall with a proactive mindset and plan of action to limit the impact of the flu and preserve hospital resources,” the Washington Examiner reported.
The caution was certainly warranted. A normal flu season strains resources, but a severe flu season coupled with a global pandemic could have been disastrous. Luckily, Ducey’s “perfect storm” did not materialize.
Data from the World Health Organization’s FluNet Global Influenza Surveillance and Response System was used by Nature to develop the graphic above. It illustrates how the number of positive Influenza specimens in 2019-2020 declined compared to the previous two years. Some experts believe this is due to protocols implemented to combat the COVID-19 coronavirus by hospitals and clinical laboratories. (Graphic copyright: Nature.)
Why Is There Less Influenza?
So, why is there less flu and other respiratory infections?
Epidemiologist Lisa Lockerd Maragakis, MD, MPH, Associate Professor of Medicine and Senior Director of Infection Prevention at Johns Hopkins Health System, told U.S. News, widespread business and school closures provide fewer opportunities for influenza to spread. “We commonly see flu spread in communities, schools, businesses and through travel each year, so those changes are likely keeping the flu away.”
However, this may have a negative effect as well. Eili Klein, PhD, Associate Professor of Emergency Medicine at Johns Hopkins School of Medicine, warns that “Because of the current restrictions and precautions everyone is taking this season, far fewer people will be infected or exposed to the flu virus, and therefore won’t become immune to certain strains of the virus. So, the number of people who may have more severe infections next year is likely to be greater because immunity will be lower,” the Washington Examiner reported.
Other Viral Infections Also in Decline Due to COVID-19 Precautions, Vaccines
Masking, frequent handwashing, and social distancing certainly played a role in reducing the number of cases of flu reported this year. But influenza is not the only disease that saw reductions. “In Hong Kong, compared with previous years, the number of chickenpox cases dropped by about half to three-quarters,” Nature reported. “In April, cases of measles and rubella were their lowest, globally, since at least 2016, according to data available so far.”
Early in the COVID-19 pandemic, some public health officials were concerned that the decline in influenza cases was actually related to a lack of testing. “However, renewed efforts by public health officials and clinicians to test samples for influenza resulted in adequate numbers tested and detection of little to no influenza virus,” the Centers for Disease Control and Prevention (CDC) reported.
Another factor in the lower numbers of flu cases could be due to the fact that more people have gotten vaccinated this year. More than 188 million flu vaccines were distributed in 2020, an increase compared to the 169 million given in 2019.
“Flu vaccination in the community started earlier this year, as recommended by the CDC, and our community physicians report that vaccine uptake has been higher than usual,” Marie-LouiseLandry, MD, Clinical Virologist, Professor of Laboratory Medicine and of Medicine (Infectious Diseases), and Director of the Clinical Virology Laboratory at Yale School of Medicine, told Healthline.
It may also be that influenza diagnoses are fewer because people are not seeking treatment. Hospitals at or beyond capacity due to the pandemic, or fear of contracting COVID-19, may have motivated people with flu-like symptoms to stay home rather than seek treatment. However, most healthcare experts agree that public health measures to fight COVID-19 are likely the larger reason there is less flu.
“Public health measures such as movement restrictions, social distancing, and increased personal hygiene likely had an effect on decreasing influenza and other respiratory virus transmissions,” the World Health Organization (WHO) told Nature.
What About the Next Flu Season?
Experts are more conflicted regarding what all of this means for coming flu seasons. Some experts think that because there’s less flu this year, there will be less immunity next year, and severe illness will result. Others are more optimistic and hope that some strains of flu will disappear, which could mean less flu in the immediate future. It’s not a simple prediction to make.
Even if the low flu numbers this year mean some strains do not survive, it is unlikely that will remain the case. “I am sure that flu will come back with a vengeance at some stage in the future,” Robert Ware, PhD, a biostatistician, clinical epidemiologist, and Professor of Biostatistics with Griffith University in Queensland, Australia, told Nature.
Thus, clinical laboratories should remain vigilant for future influenza outbreaks. Hopefully by then the COVID-19 pandemic will have peaked and labs will be able to reallocate testing resources appropriately.
Pathologists and clinical laboratory scientists know that influenza vaccines typically produce short-lived protection and researchers have new clues as to why this is true
With so much interest in development of a COVID-19 vaccine, findings by researchers at Atlanta’s Emory Vaccine Center into why the vaccine for influenza (Flu) is so short-lived offer a new window on how the body’s immune system responds to invading viruses and what happens to the immunity over time.
Because the autumn influenza season is just weeks away, these insights into the body’s immune response to influenza will be of interest to clinical laboratories that provide testing for influenza, as well as SARS-CoV-2, the coronavirus that causes COVID-19.
Clinical laboratory managers recognize that an influenza vaccine is an annual imperative for people—especially the elderly and those with existing comorbidities—and medical laboratory tests are typically used to diagnose the illness and identify which strains of viruses are present. The flu vaccine is even more important amid the COVID-19 pandemic, infectious disease authorities say.
The scientists at the Emory Vaccine Center published their findings in the journal Science.
Not so with influenza vaccines. The immunity they impart generally only lasts for a single flu season and are “lost within one year,” the Emory study notes.
As Genetic Engineering and Biotechnology News (GEN) explains, the influenza genome has eight RNA segments which can change as the virus enters a cell. This antigenic shift creates new influenza strains that require updated vaccines, GEN noted.
However, the Emory researchers stated that “The fact that a small number did persist over one year raises prospects that the longevity of flu vaccines can be improved and provides key information for the development of universal vaccines against influenza.”
Bone Marrow Has Major Role in Producing New Flu Antibodies
The Emory study focused on the influenza vaccine’s role in how it affects the immune system and what needs to change to create a longer-lasting influenza vaccine. “Our results suggest that most bone marrow plasma cells (BMPC) generated by influenza vaccination in adults are short-lived. Designing strategies to enhance their persistence will be key,” the Emory researchers wrote in Science.
The scientists analyzed bone marrow from 53 healthy volunteers (age 20 to 45). An Emory news release states that bone marrow is the “home base for immune cells producing antibodies.”
Besides the bone marrow, the researchers also examined blood samples from the volunteers, all of which was collected between 2009 and 2018:
before influenza vaccination,
one month after influenza vaccination, and
one year post vaccination.
Through DNA sequencing the samples, the Emory researchers found the number of flu-specific cells increased from 0.8% to 1.9% after one month. They concluded that an annual vaccine does increase antibody-producing cells for influenza in bone marrow.
However, in follow-up visits one year after vaccination, they found that the number of cells present in the volunteers had fallen back to the starting point.
“Specific cells produced by the vaccine … produced unique antibodies that can be identified using sequencing techniques,” Carl Davis, PhD, postdoctoral fellow in the Rafi Ahmed Laboratory at Emory and first author of the paper, said in the news release, adding, “We could see that these new antibodies expanded in the bone marrow one month after vaccination and then contracted after one year.”
He continued, “On the other hand, antibodies against influenza that were in the bone marrow before the vaccine was given stayed at a constant level over one year.”
Vaccine Adjuvants Help Boost Immunity
A vaccine additive called an adjuvant could be the answer to extending the power of influenza vaccines, the Emory scientists noted.
“Just getting to the bone marrow is not enough. A plasma cell has to find a niche within the bone marrow and establish itself there and undergo gene expression and metabolism changes that promote longevity,” Rafi Ahmed, PhD, Director of the Emory Vaccine Center, said in the news release.
“It’s totally crazy (that the most commonly used influenza vaccines don’t include an adjuvant), Ahmed told Science. “I’m hoping that things will change in the influenza vaccine world, and 10 years from now, you will not be getting any nonadjuvanted vaccines.”
According to USA Today, about 20-million “essential” workers will likely be the first to receive the new COVID-19 vaccine and participate in check-in text messages with the Centers for Disease Control and Prevention (CDC) by the end of 2020.
In its COVID-19 vaccine testing, Novavax, a late-state biotechnology company, suggests that “an adjuvant is critical to its vaccine working well,” National Public Radio (NPR) reported in “The Special Sauce That Makes Some Vaccines Work.” However, vaccine developers may be reluctant to share their adjuvant research.
“Adjuvants end up being very proprietary. It’s kind of the secret sauce on how to make your protein vaccine work,” Barney Graham, MD, PhD, Deputy Director, Vaccine Research Center, National Institute of Allergy and Infectious Diseases, told NPR.
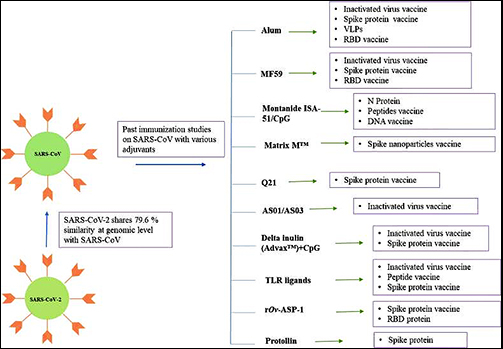
Still, a study published in Immunopharmacology revealed potential adjuvants for the COVID-19 vaccine based on vaccine studies of other coronaviruses. While there are many adjuvants available, not all have safety track records that can be leveraged to gain clearance from regulatory bodies, the researchers pointed out. But some do.
“CpG 1018, MF59, and AS03 are already approved for human vaccine and their inclusion may expedite the vaccine development process. Further, Protollin has shown promising results in pre-clinical studies,” the authors wrote.
Clinical laboratories that provide influenza testing will want to follow these types of research studies. Findings on immunity will affect development of vaccines that medical labs provide—including for COVID-19.
As standard masks are used they collect exhaled airborne pathogens that remain living in the masks’ fibers, rendering them infectious when handled
Surgical-style facial masks harbor a secret—viruses that could be infectious to the people wearing them. However, masks can become effective virus killers as well. At least that’s what researchers at the University of Alberta (UAlberta) in Edmonton, Canada, have concluded.
If true, such a re-engineered mask could protect clinical laboratory workers from exposure to infectious diseases, such as, SARS (Severe Acute Respiratory Syndrome), MERS (Middle East Respiratory Syndrome), and Swine Influenza.
“Surgical masks were originally designed to protect the wearer from infectious droplets in clinical settings, but it doesn’t help much to prevent the spread of respiratory diseases such as SARS or MERS or influenza,” Hyo-Jick Choi, PhD, Assistant Professor in UAlberta’s Department of Chemical and Materials Engineering, noted in a press release.
So, Choi developed a mask that effectively traps and kills airborne viruses.
Clinical Laboratory Technicians at Risk from Deadly Infectious Diseases
The global outbreak of SARS in 2003 is a jarring reminder of how infectious diseases impact clinical laboratories, healthcare workers, and patients. To prevent spreading the disease, Canadian-based physicians visited with patients in hotel rooms to keep the virus from reaching their medical offices, medical laboratory couriers were turned away from many doctors’ offices, and hospitals in Toronto ceased elective surgery and non-urgent services, reported The Dark Report—Dark Daily’s sister publication. (See The Dark Report, “SARS Challenges Met with New Technology,” April 14, 2003.)
UAlberta materials engineering professor Hyo-Jick Choi, PhD, (right) and graduate student Ilaria Rubino (left) examine filters treated with a salt solution that kills viruses. Choi and his research team have devised a way to improve the filters in surgical masks, so they can trap and kill airborne pathogens. Clinical laboratory workers will especially benefit from this protection. (Photo and caption copyright: University of Alberta.)
How Current Masks Spread Disease
How do current masks spread infectious disease? According to UAlberta researchers:
A cough or a sneeze transmits airborne pathogens such as influenza in aerosolized droplets;
Virus-laden droplets can be trapped by the mask;
The virus remains infectious and trapped in the mask; and,
Risk of spreading the infection persists as the mask is worn and handled.
“Aerosolized pathogens are a leading cause of respiratory infection and transmission. Currently used protective measures pose potential risk of primary and secondary infection and transmission,” the researchers noted in their paper, published in Scientific Reports.
That’s because today’s loose-fitting masks were designed primarily to protect healthcare workers against large respiratory particles and droplets. They were not designed to protect against infectious aerosolized particles, according to the Centers for Disease Control and Prevention (CDC).
In fact, the CDC informed the public that masks they wore during 2009’s H1N1 influenza virus outbreak provided no assurance of infection protection.
“Face masks help stop droplets from being spread by the person wearing them. They also keep splashes or sprays from reaching the mouth and nose of the person wearing the face mask. They are not designed to protect against breathing in very small particle aerosols that may contain viruses,” a CDC statement noted.
Pass the Salt: A New Mask to Kill Viruses
Choi and his team took on the challenge of transforming the filters found on many common protective masks. They applied a coating of salt that, upon exposure to virus aerosols, recrystallizes and destroys pathogens, Engineering360 reported.
“Here we report the development of a universal, reusable virus deactivation system by functionalization of the main fibrous filtration unit of surgical mask with sodium chloride salt,” the researchers penned in Scientific Reports.
The researchers exposed their altered mask to the influenza virus. It proved effective at higher filtration compared to conventional masks, explained Contagion Live. In addition, viruses that came into contact with the salt-coated fibers had more rapid infectivity loss than untreated masks.
How Does it Work?
Here’s how the masks work, according to the researchers:
Aerosol droplets carrying the influenza virus contact the treated filter;
The droplet absorbs salt on the filter;
The virus is exposed to increasing concentration of salt; and,
The virus is damaged when salt crystallizes.
“Salt-coated filters proved highly effective in deactivating influenza viruses regardless of [influenza] subtypes,” the researchers wrote in Scientific Reports. “We believe that [a] salt-recrystallization-based virus deactivation system can contribute to global health by providing a more reliable means of preventing transmission and infection of pandemic or epidemic diseases and bioterrorism.”
Other Reports on Dangerous Exposure for Clinical Laboratory Workers
This is not the first time Dark Daily has reported on dangers to clinical laboratory technicians and ways to keep them safe.
In “Health of Pathology Laboratory Technicians at Risk from Common Solvents like Xylene and Toluene,” we reported on a 2011 study that determined medical laboratory technicians who handle common solvents were at greater risk of developing auto-immune connective tissue diseases.
The UAlberta team may have come up with an inexpensive, simple, and effective way to protect healthcare workers and clinical laboratory technicians. Phlebotomists, laboratory couriers, and medical technologists also could wear the masks as protection from accidental infection and contact with specimens. It will be interesting to follow the progress of this special mask with its salty filter.
Mounting financial and patient-care problems in UK show NHS may not provide a quality blueprint for fixing US healthcare system flaws
Patients scheduled for elective surgeries—such as hip replacements or penciled in for routine outpatient appointments—have been turned away this winter from National Health Service (NHS) hospitals as the United Kingdom’s (UK’s) public healthcare system suffers another care emergency.
This latest crisis in the UK should provide further evidence to anatomic pathologists and medical laboratory leaders that the United States healthcare system is not alone in facing mounting financial and patient care questions. While an NHS-like single-payer healthcare system in the US is the goal of many reformers, the UK’s current crisis indicates such a system has serious flaws.
UK News Organizations Disagree with Government Leaders as to Cause of Crisis
NHS officials estimate as many as 55,000 elective operations and outpatient procedures were cancelled as hospitals attempted to free up capacity for the sickest patients. The Telegraph reported that the bed shortfall is blamed on a spike in winter flu, with budget cuts to social services for home healthcare, staff shortages, and an aging population further pressuring the healthcare system.
In late January, the NHS’ National Emergency Pressure Panel (NEPP) announced that planned operations, such as elective surgeries, that had been “suspended because of pressure on the NHS in January,” would be able to resume in February, Sky News reported.
Meanwhile, in response to the original decision in January to have hospitals stop performing elective surgeries and similar procedures, an editorial in The Guardian challenged Prime Minister Theresa May’s suggestion that the current crisis was primarily due to the flu epidemic.
“This is not the flu: it is a system-wide crisis brought about by seven years of mounting austerity,” The Guardian’s editors wrote. “Oh, and that is getting worse, too. The official defense is that this is not a crisis because there is a plan … But planning can’t magic up highly trained doctors and nurses. Plans do not make hospital beds. And while vaccination helps, you can’t entirely plan your way out of the impact of flu.”
Doctors Report ‘Intolerable Conditions’ at 68 Hospitals
The crisis reached new heights when specialists in emergency medicine from 68 hospitals sent a letter to the prime minister stating the “current level of safety compromise is at times intolerable, despite the best efforts of staff.” The letter, published in The Guardian, also pointed out media coverage reporting anecdotal accounts of “appalling” situations in many emergency departments “are not outliers.” According the doctors, conditions include:
Over 120 patients a day managed in corridors, some dying prematurely;
An average of 10-12 hours from decision to admit a patient until they are transferred to a bed;
Over 50 patients at a time awaiting beds in the emergency department; and,
Patients sleeping in clinics as makeshift wards.
One doctor, Richard Fawcett, MD, drew media attention when he used Twitter to apologized for “third world conditions” caused by overcrowding in the hospital where he works, The Telegraph reported.
Richard Fawcett, MD (above), a consultant in emergency medicine for University Hospitals of North Midlands NHS Trust, drew widespread media attention in England when he apologized to patients on Twitter for the “third world conditions” this winter at the hospital where he works. A Lieutenant Colonel in the British Royal Army, Fawcett has done three deployments to Afghanistan. (Photo copyright: Midlands Air Ambulance Charity.)
NHS officials acknowledged staff criticism but attempted to paint the crisis as temporary. University of North Midlands NHS Trust (UHNM) told BBC News that area hospitals had been under “severe and sustained pressure over the Christmas period,” which had “continued into the new year.”
“Our staff want the very best for our patients and at times they find the situation frustrating, which can be reflected on social media. However, we are a leading trauma, stroke, and cardiac center and have been regularly praised by external independent commentators for the quality of compassionate care provided at our hospitals despite all our pressures,” Dr. John Oxtoby, Consultant Radiologist and Deputy Medical Director, UHNM, told BBC News.
“We have to keep going and turn up in a fit state to do the best job that we can. But it’s been really tough, particularly on more junior staff,” one hospital staff member told The Guardian. “And when they ask me, ‘Will it always be like this and will it get better?’ I cannot say it will improve as the truth is it won’t unless the NHS gets the resources and investment it needs.”
Basic Elements of Care Neglected
This is not the first time the NHS has come under fire for substandard patient care.
Between 400 and 1,200 patients are estimated to have died as result of poor care between January 2005 and March 2008 at Stafford Hospital, reported The Guardian. A 2010 report into care at the hospital, now named County Hospital and run by UHNM, found a litany of problems.
“For many patients, the most basic elements of care were neglected,” inquiry Chairman Sir Robert Francis, QC, told The Guardian. “Some patients needing pain relief either got it late or not at all. Others were left unwashed for up to a month … The standards of hygiene were at times awful, with families forced to remove used bandages and dressings from public areas and clean toilets themselves for fear of catching infections.”
Reports of substandard patient care within the United Kingdom’s National Health Service are not new. British barrister Sir Robert Francis, QC (above), led investigations into the Stafford Hospital scandal, which uncovered that an estimated 400 to 1200 patients died between 2005 and 2008 at the facility due to appalling conditions and lax procedures. (Photo copyright: The Telegraph.)
Why not this crisis in US? Because, even if our system of healthcare has flaws, it is responsive to consumer/patient demand. Whereas, in the UK, the NHS is always budget short and so is always struggling to invest in expanding hospital/physician capacity to meet the steady increase in patient demand.
Dark Daily’s goal in reporting on this story is to help anatomic pathologists and clinical laboratory leaders in the United States understand that every country’s health system—like ours—has its share of unique problems and is not perfect.