Japanese scientists who developed the detection method hope to use it to create ‘easy testing kits that anyone can use’
What do ostriches and humans have in common during the current COVID-19 pandemic? The unexpected answer is that ostrich antibodies can be used to identify humans infected with COVID-19. If proven viable in healthcare settings, the possibility exists that new clinical laboratory tests could be developed based on wearable diagnostics technologies that pathologists would interpret for doctors and patients.
According to Study Finds, scientists at Kyoto Prefectural University in Japan have created a removable mask filter that, when sprayed with a fluorescent dye coated with antibodies extracted from ostrich eggs, will glow under UV light when COVID-19 is detected. The discovery by Yasuhiro Tsukamoto, PhD (above), President of Kyoto Prefectural University, and his researchers could lead to development of low-cost at home COVID-19 testing kits using the same ostrich-antibody-based technique. (Photo copyright: Kyoto Prefectural University/Reuters.)
The KPU scientists conducted a small study with 32 COVID-19 patients over a 10-day span. The surgical-style masks they wore later glowed around the nose and mouth areas but became dimmer over time as their viral load decreased.
“The ostrich antibody for corona placed on the mouth filter of the mask captures the coronavirus in coughing, sneezing, and water,” the researchers explained in Study Finds.
Tsukamoto himself learned he had contracted COVID-19 after wearing a prototype mask and noticing it glowed under UV light. A PCR test later confirmed his diagnosis, Kyodo News reported.
The KPU team “hopes to further develop the masks so they will glow automatically, without special lighting, if the [COVID-19] virus is detected.” Reuters noted in its coverage of the ostrich-antibody masks.
Making Medicine from Ostrich Antibodies
A profile in Audubon noted that Tsukamoto, who also serves as a veterinary medicine professor at Kyoto Prefectural University, made ostriches the focus of his research since the 1990s as he looked for ways to harness the dinosaur-like bird’s properties to fight human infections. He maintains a flock of 500 captive ostriches. Each female ostrich can produce 50 to 100 eggs/year over a 50-year life span.
Tsukamoto’s research focuses on customizing the antibodies in ostrich eggs by injecting females with inactive viruses, allergens, and bacteria, and then extracting the antibodies to develop medicines for humans. Antibodies form in the egg yolks in about six weeks and can be collected without harming the parent or young.
“The idea of using ostrich antibodies for therapeutics in general is a very interesting concept, particularly because of the advantages of producing the antibodies from eggs,” Ashley St. John, PhD, an Associate Professor in Immunology, at Duke-NUS Medical School in Singapore, told Audubon.
While more clinical studies will be needed before ostrich-antibody masks reach the commercial marketplace, Tsukamoto’s team is planning to expand their experiment to 150 participants with a goal of receiving Japanese government approval to begin selling the glowing COVID-detection masks as early as 2022. But they believe the ostrich-antibody technique ultimately may lead to development of an inexpensive COVID-19 testing kit.
“We can mass-produce antibodies from ostriches at a low cost. In the future, I want to make this into an easy testing kit that anyone can use,” Tsukamoto told Kyodo News.
Harvard, MIT Also Working on COVID-19 Detecting Facemask
According to Fast Company, the MIT/Harvard COVID-19-detecting masks use the same core technology as previous paper tests for Ebola and Zika that utilize proteins and nucleic acids embedded in paper that react to target molecules.
Fast Company explained that the mask wearer launches a test by pushing a button to release a small water reservoir embedded in the mask (above). Droplets from their breath are than analyzed by the sensors in the masks, which could be adapted to test for new COVID variants or other respiratory pathogens. In addition to eliminating the use of a nasal swab, the mask-based testing system may compete with clinical laboratory-based results. (Photo copyright: Felice Frankel/MIT.)
“They would especially be useful in situations where local variant outbreaks are occurring, allowing people to conveniently test themselves at home multiple times a day,” he told Fast Company.
“It’s on par specificity and sensitivity that you will get in a state-of-the-art [medical] laboratory, but with no one there,” Luis Ruben Soenksen, PhD, Venture Builder in Artificial Intelligence and Healthcare at MIT and one of the co-authors of the Nature Biotechnology study, told Fast Company.
As the definition of “wearable diagnostic technology” broadens, pathologists and clinical laboratory scientists may see their roles expand to include helping consumers interpret data collected by point-of-care testing technology as well as performing, evaluating, and interpreting laboratory test results that come from non-traditional sources.
MIT’s deep learning artificial intelligence algorithm demonstrates how similar new technologies and smartphones can be combined to give dermatologists and dermatopathologists valuable new ways to diagnose skin cancer from digital images
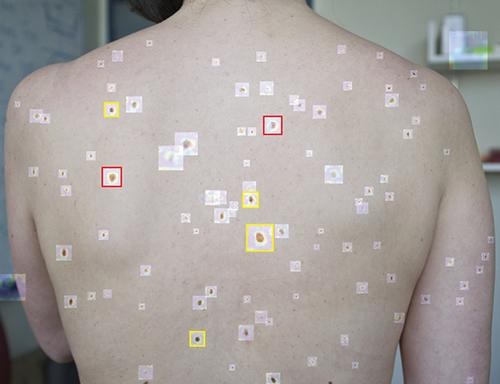
According to an MIT press release, “The paper describes the development of an SPL [Suspicious Pigmented Lesion] analysis system using DCNNs [Deep Convolutional Neural Networks] to more quickly and efficiently identify skin lesions that require more investigation, screenings that can be done during routine primary care visits, or even by the patients themselves. The system utilized DCNNs to optimize the identification and classification of SPLs in wide-field images.”
The MIT scientists believe their AI analysis system could aid dermatologists, dermatopathologists, and clinical laboratories detect melanoma, a deadly form of skin cancer, in its early stages using smartphones at the point-of-care.
“Our research suggests that systems leveraging computer vision and deep neural networks, quantifying such common signs, can achieve comparable accuracy to expert dermatologists,” said Luis Soenksen, PhD (above), Venture Builder in Artificial Intelligence and Healthcare at MIT and first author of the study in an MIT press release. “We hope our research revitalizes the desire to deliver more efficient dermatological screenings in primary care settings to drive adequate referrals.” The MIT study demonstrates that dermatologists, dermatopathologists, and clinical laboratories can benefit from using common technologies like smartphones in the diagnosis of disease. (Photo copyright: Wyss Institute Harvard University.)
Improving Melanoma Treatment and Patient Outcomes
Melanoma develops when pigment-producing cells called melanocytes start to grow out of control. The cancer has traditionally been diagnosed through visual inspection of SPLs by physicians in medical settings. Early-stage identification of SPLs can drastically improve the prognosis for patients and significantly reduce treatment costs. It is common to biopsy many lesions to ensure that every case of melanoma can be diagnosed as early as possible, thus contributing to better patient outcomes.
“Early detection of SPLs can save lives. However, the current capacity of medical systems to provide comprehensive skin screenings at scale are still lacking,” said Luis Soenksen, PhD, Venture Builder in Artificial Intelligence and Healthcare at MIT and first author of the study in the MIT press release.
The researchers trained their AI system by using 20,388 wide-field images from 133 patients at the Gregorio Marañón General University Hospital in Madrid, as well as publicly available images. The collected photographs were taken with a variety of ordinary smartphone cameras that are easily obtainable by consumers.
They taught the deep learning algorithm to examine various features of skin lesions such as size, circularity, and intensity. Dermatologists working with the researchers also visually classified the lesions for comparison.
When the algorithm is “shown” a wide-field image like that above taken with a smartphone, it uses deep convolutional neural networks to analyze individual pigmented lesions and screen for early-stage melanoma. The algorithm then marks suspicious images as either yellow (meaning further inspection should be considered) or red (indicating that further inspection and/or referral to a dermatologist is required). Using this tool, dermatopathologists may be able to diagnose skin cancer and excise it in-office long before it becomes deadly. (Photo copyright: MIT.)
“Our system achieved more than 90.3% sensitivity (95% confidence interval, 90 to 90.6) and 89.9% specificity (89.6 to 90.2%) in distinguishing SPLs from nonsuspicious lesions, skin, and complex backgrounds, avoiding the need for cumbersome individual lesion imaging,” the MIT researchers noted in their Science Translational Medicine paper.
In addition, the algorithm agreed with the consensus of experienced dermatologists 88% of the time and concurred with the opinions of individual dermatologists 86% of the time, Medgadget reported.
Modern Imaging Technologies Will Advance Diagnosis of Disease
According to the American Cancer Society, about 106,110 new cases of melanoma will be diagnosed in the United States in 2021. Approximately 7,180 people are expected to die of the disease this year. Melanoma is less common than other types of skin cancer but more dangerous as it’s more likely to spread to other parts of the body if not detected and treated early.
More research is needed to substantiate the effectiveness and accuracy of this new tool before it could be used in clinical settings. However, the early research looks promising and smartphone camera technology is constantly improving. Higher resolutions would further advance development of this type of diagnostic tool.
In addition, MIT’s algorithm enables in situ examination and possible diagnosis of cancer. Therefore, a smartphone so equipped could enable a dermatologist to diagnose and excise cancerous tissue in a single visit, without the need for biopsies to be sent to a dermatopathologist.
Currently, dermatologists refer a lot of skin biopsies to dermapathologists and anatomic pathology laboratories. An accurate diagnostic tool that uses modern smartphones to characterize suspicious skin lesions could become quite popular with dermatologists and affect the flow of referrals to medical laboratories.
Unlike most other CRISPR/Cas-9 therapies that are ex vivo treatments in which cells are modified outside the body, this study was successful with an in vivo treatment
Use of CRISPR-Cas9 gene editing technology for therapeutic purposes can be a boon for clinical laboratories. Not only is this application a step forward in the march toward precision medicine, but it can give clinical labs the essential role of sequencing a patient’s DNA to help the referring physician identify how CRISPR-Cas9 can be used to edit the patient’s DNA to treat specific health conditions.
Most pathologists and medical lab managers know that CRISPR-Cas9 gene editing technology has been touted as one of the most significant advances in the development of therapies for inherited genetic diseases and other conditions. Now, a pair of biotech companies have announced a milestone for CRISPR-Cas9 with early clinical data involving a treatment delivered intravenously (in vivo).
As with other therapies, determining which patients are suitable candidates for specific treatments is key to the therapy’s success. Therefore, clinical laboratories will play a critical role in identifying those patients who would most likely benefit from a CRISPR-delivered therapy.
Such is the goal of precision medicine. As methods are refined that can correct unwelcome genetic mutations in a patient, the need to do genetic testing to identify and diagnose whether a patient has a specific gene mutation associated with a specific disease will increase.
Cleveland Clinic describes ATTR amyloidosis as a “protein misfolding disorder” involving transthyretin (TTR), a protein made in the liver. The disease leads to deposits of the protein in the heart, nerves, or other organs.
According to Intellia and Regeneron, NTLA-2001 is designed to inactivate the gene that produces the protein.
The interim clinical trial data indicated that one 0.3 mg per kilogram dose of the therapy reduced serum TTR by an average of 87% at day 28. A smaller dose of 0.1 mg per kilogram reduced TTR by an average of 52%. The researchers reported “few adverse events” in the six study patients, “and those that did occur were mild in grade.”
Current treatments, the companies stated, must be administered regularly and typically reduce TTR by about 80%.
“These are the first ever clinical data suggesting that we can precisely edit target cells within the body to treat genetic disease with a single intravenous infusion of CRISPR,” said Intellia President and CEO John Leonard, MD, in a press release. “The interim results support our belief that NTLA-2001 has the potential to halt and reverse the devastating complications of ATTR amyloidosis with a single dose.”
He added that “solving the challenge of targeted delivery of CRISPR-Cas9 to the liver, as we have with NTLA-2001, also unlocks the door to treating a wide array of other genetic diseases with our modular platform, and we intend to move quickly to advance and expand our pipeline.”
“It’s an important moment for the field,” MIT biomedical engineer Daniel Anderson, PhD (above), told Nature. Anderson is Professor, Chemical Engineering and Institute for Medical Engineering and Science at the Koch Institute for Integrative Cancer Research at MIT. “It’s a whole new era of medicine,” he added. Advances in the use of CRISPR-Cas9 for therapeutic purposes will create the need for clinical laboratories to sequence patients’ DNA to help physicians determine the best uses for a CRISPR-Cas9 treatment protocol. (Photo copyright: Massachusetts Institute of Technology.)
In Part 2 of the Phase 1 trial, Intellia plans to evaluate the new therapy at higher doses. After the trial is complete, “the company plans to move to pivotal studies for both polyneuropathy and cardiomyopathy manifestations of ATTR amyloidosis,” the press release states.
Previous clinical trials reported results for ex vivo treatments in which cells were removed from the body, modified with CRISPR-Cas9 techniques, and then reinfused. “But to be able to edit genes directly in the body would open the door to treating a wider range of diseases,” Nature reported.
How CRISPR-Cas9 Works
On its website, CRISPR Therapeutics, a company co-founded by Emmanuelle Charpentier, PhD, a director at the Max Planck Institute for Infection Biology in Berlin, and inventor of CRISPR-Cas9 gene editing, explained that the technology “edits genes by precisely cutting DNA and then letting natural DNA repair processes take over.” It can remove fragments of DNA responsible for causing diseases, as well as repairing damaged genes or inserting new ones.
The therapies have two components: Cas9, an enzyme that cuts the DNA, and Guide RNA (gRNA), which specifies where the DNA should be cut.
Charpentier and biochemist Jennifer Doudna, PhD, Nobel Laureate, Professor of Chemistry, Professor of Biochemistry and Molecular Biology, and Li Ka Shing Chancellor’s Professor in Biomedical and Health at the University of California Berkeley, received the 2020 Nobel Prize in Chemistry for their work on CRISPR-Cas9, STAT reported.
It is important to pathologists and medical laboratory managers to understand that multiple technologies are being advanced and improved at a remarkable pace. That includes the technologies of next-generation sequencing, use of gene-editing tools like CRISPR-Cas9, and advances in artificial intelligence, machine learning, and neural networks.
At some future point, it can be expected that these technologies will be combined and integrated in a way that allows clinical laboratories to make very early and accurate diagnoses of many health conditions.
Use of such precision diagnostics offer ‘early detection, localization, and the opportunity to monitor response to therapy,’ say the MIT scientists
Oncologists and medical laboratory scientists know that most clinical laboratory tests currently used to diagnose cancer are either based on medical imaging technologies—such as CT scans and mammography—or on molecular diagnostics that detect cancer molecules in the body’s urine or blood.
Now, in a study being conducted at the Massachusetts Institute of Technology (MIT), researchers have developed diagnostic nanoparticles that can not only detect cancer cells in bodily fluids but also image the cancer’s location. This is the latest example of how scientists are combining technologies in new ways in their efforts to develop more sensitive diagnostic tests that clinical laboratories and other providers can use to detect cancer and other health conditions.
Precision diagnostics such as molecular, imaging, and analytics technologies are key tools in the pursuit of precision medicine.
“Therapeutic outcomes in oncology may be aided by precision diagnostics that offer early detection, localization, and the opportunity to monitor response to therapy,” the authors wrote, adding, “Through tailored target specificities, this modular platform has the capacity to be engineered as a pan-cancer test that may guide treatment decisions for numerous tumor type.”
Development of Multimodal Diagnostics
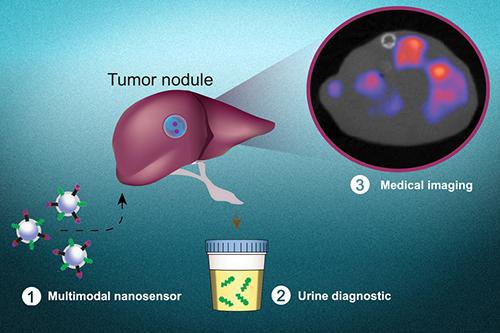
The MIT scientists are developing a “multimodal” diagnostic that uses molecular screening combined with imaging techniques to locate where a cancer began in the body and any metastases that are present.
“In principle, this diagnostic could be used to detect cancer anywhere in the body, including tumors that have metastasized from their original locations,” an MIT new release noted.
“This is a really broad sensor intended to respond to both primary tumors and their metastases,” said biological engineer Sangeeta Bhatia, MD, PhD (above), in the news release. Bhatia is the John and Dorothy Wilson Professor of Health Sciences and Technology and Electrical Engineering and Computer Science at MIT and senior author of the study.
“It can trigger a urinary signal and also allow us to visualize where the tumors are,” she added. Bhatia previously worked on the development of cancer diagnostics that can produce synthetic biomarkers which are detectable in urine samples.
“The vision is that you could use this in a screening paradigm—alone or in conjunction with other tests—and we could collectively reach patients that do not have access to costly screening infrastructure today,” said Sangeeta Bhatia, MD, PhD (above), in the MIT news release. “Every year you could get a urine test as part of a general check-up. You would do an imaging study only if the urine test turns positive to then find out where the signal is coming from. We have a lot more work to do on the science to get there, but that’s where we would like to go in the long run.” (Photo copyright: NBC News.)
Precision Diagnostic Assists Assessment of Response to Cancer Therapy
For their research, the scientists added a radioactive tracer known as copper-64 to the nanoparticles. This enabled the particles to be used for positron emission tomography (PET) imaging. The particles were coated with a peptide that induced them to accumulate at tumor sites and insert themselves into cell membranes, producing a strong imaging signal for tumor detection.
The researchers tested their diagnostic nanoparticles in mouse models of metastatic colon cancer where tumor cells had traversed to the liver or the lungs. After treating the cancer cells with a chemotherapy regimen, the team successfully used both urine and imaging to determine how the tumors were responding to the treatment.
Bhatia is hopeful that this type of diagnostic could be utilized in assessing how patients are responding to treatment therapies and the monitoring of tumor recurrence or metastasis, especially for colon cancer.
What is unique about the approach used by Bhatia’s team is that one application of the copper-64 tracer can be used in vivo, in combination with imaging technology. The other application of the copper-64 tracer is in vitro in a urine specimen that can be tested by clinical laboratories.
“Those patients could be monitored with the urinary version of the test every six months, for instance. If the urine test is positive, they could follow up with a radioactive version of the same agent for an imaging study that could indicate where the disease had spread,” Bhatia said in the news release. “We also believe the regulatory path may be accelerated with both modes of testing leveraging a single formulation.”
The graphic above, taken from the MIT news release, shows how “multimodal nanosensors (1) are engineered to target and respond to hallmarks in the tumor microenvironment. The nanosensors provide both a noninvasive urinary monitoring tool (2) and an on-demand medical imaging agent (3) to localize tumor metastasis and assess response to therapy,” the news release states. (Photo and caption copyright: Massachusetts Institute of Technology.)
Precision Medicine Cancer Screening Using Nano Technologies
Bhatia hopes that the nanoparticle technology may be used as a screening tool in the future to detect any type of cancer.
Her previous research with nanoparticle technology determined that a simple urine test could diagnose bacterial pneumonia and indicate if antibiotics could successfully treat that illness, the news release noted.
Nanoparticle-based technology might be adapted in the future to be part of a screening assay that determines if cancer cells are present in a patient. In such a scenario, clinical laboratories would be performing tests on urine samples while imaging techniques are simultaneously being used to diagnose and monitor cancers.
Surgical pathologists may also want to monitor the progress of this research, as it has the potential to be an effective tool for monitoring cancer patients following surgery, chemotherapy, or radiation therapy.
AccuWeather interviewed experts, including pathologists who have analyzed the virus, who say SARS-CoV-2 is susceptible to heat, light, and humidity, while others study weather patterns for their predictions
AccuWeather, as it watched the outbreak of SARS-CoV-2, the novel coronavirus that causes COVID-19, wanted to know what effect that warmer spring temperatures might have on curbing the spread of the virus. There is a good reason to ask this question. As microbiologists, infectious disease doctors, and primary care physicians know, the typical start and end to every flu season is well-documented and closely watched.
As SARS-CoV-2 ravages countries around the world, clinical pathologists and microbiologists debate whether it will subside as temperatures rise in Spring and Summer. Recent analyses suggest it may indeed be a seasonal phenomenon. However, some infectious disease specialists have expressed skepticism.
CNN reported that Nicholls was part of a research team which reproduced the virus in January to study its behavior and evaluate diagnostic tests. Nicholls was also involved in an early effort to analyze the coronavirus associated with the 2003 SARS outbreak involving SARS-CoV, another coronavirus that originated in Asia.
“Sunlight will cut the virus’ ability to grow in half, so the half-life will be 2.5 minutes and in the dark it’s about 13 to 20,” Nicholls told AccuWeather. “Sunlight is really good at killing viruses.” And that, “In cold environments, there is longer virus survival than warm ones.” He added, “I think it will burn itself out in about six months.”
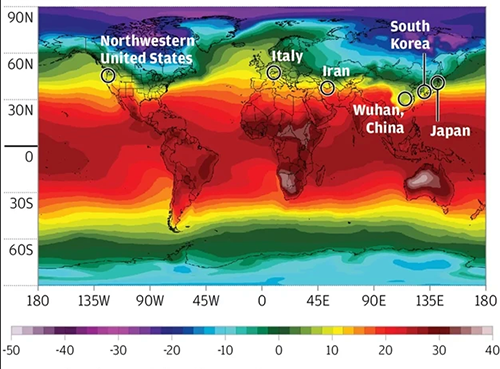
The graphic above, created by John Nicholls, MBBS Adel, FRCPA, FHKCPath, FHKAM (Pathology), Clinical Professor of Pathology at the University of Hong Kong, shows “the temperate zone where the major SARS-CoV-2 hotspots have appeared so far. The variation from year to year, in this case, is minimal; however, meteorologists would typically use the 30-year normal data for this type of analysis.” (Caption and graphic copyright: AccuWeather/John Nicholls.)
Can Weather Predict the Spread of COVID-19?
Other researchers have analyzed regional weather data to see if there’s a correlation with incidence of COVID-19. A team at the Massachusetts Institute of Technology (MIT) found that the number of cases has been relatively low in areas with warm, humid conditions and higher in more northerly regions. They published their findings in SSRN (formerly Social Science Research Network), an open-access journal and repository for early-stage research, titled “Will Coronavirus Pandemic Diminish by Summer?”
FREE Webinar | What Hospital and Health System Labs Need to Know About Operational Support and Logistics During the COVID-19 Outbreak Wednesday, April 1, 2020 @ 1PM EDT — Register or Stream now
The MIT researchers found that as of March 22, 90% of the
transmissions of SARS-CoV-2 occurred within a temperature range of three to 17
degrees Celsius (37.4 to 62.6 degrees Fahrenheit) and an absolute humidity
range of four to nine grams per cubic meter. Fewer than 6% of the transmissions
have been in warmer climates further south, they wrote.
“Based on the current data on the spread of [SARS-CoV-2], we
hypothesize that the lower number of cases in tropical countries might be due
to warm humid conditions, under which the spread of the virus might be slower
as has been observed for other viruses,” they wrote.
In the US, “the outbreak also shows a north-south divide,”
with higher incidence in northern states, they wrote. The outliers are Oregon,
with fewer than 200 cases, and Louisiana, where, as of March 22, approximately
1,000 had been reported.
There’s been a recent spike in reported cases from warmer
regions in Asia, South America, and Africa, but the MIT researchers attribute
this largely to increased testing.
Still, “there may be several caveats to our work,” they
wrote in their published study. For example, South Korea has been engaged in
widespread testing that includes asymptomatic individuals, whereas other
countries, including the US, have limited testing to a narrower range of
people, which could mean that more cases are going undetected. “Further, the
rate of outdoor transmission versus indoor and direct versus indirect
transmission are also not well understood and environmental related impacts are
mostly applicable to outdoor transmissions,” the MIT researchers wrote.
Even in warmer, more humid regions, they advocate “proper
quarantine measures” to limit the spread of the virus.
The New York Times (NYT) reported that other recent studies have shown a correlation between weather conditions and the incidence of COVID-19 outbreaks as well, though none of this research has been peer reviewed.
Why the Correlation? It’s Unclear, MIT Says
Though the MIT researchers found a strong relation between
the number of cases and weather conditions, “the underlying reasoning behind
this relationship is still not clear,” they wrote. “Similarly, we do not know
which environmental factor is more important. It could be that either
temperature or absolute humidity is more important, or both may be equally or
not important at all in the transmission of [SARS-CoV-2].”
Some experts have looked at older coronaviruses for clues. “The coronavirus is surrounded by a lipid layer, in other words, a layer of fat,” said molecular virologist Thomas Pietschmann, PhD, Director of the Department for Experimental Virology at the Helmholtz Center for Infection Research in Hanover, Germany, in a story from German news service Deutsche Welle. This makes it susceptible to temperature increases, he suggested.
However, Pietschmann cautioned that because it’s a new
virus, scientists cannot say if it will behave like older viruses. “Honestly
speaking, we do not know the virus yet,” he concluded.
Epidemiologist and virologist Joseph Fair, PhD, MPH (above), Special Advisor for Ebola, USAID, and Research Professor at Texas A&M University, said that sunlight might be a bigger factor than temperature or humidity. “It really doesn’t have anything to do with the warmth, but it has to do with the length of the day and the exposure to sunlight which inactivates the virus through UV light,” he told NBC News. “The science is still out,” he said. “We can assume this will follow typical other coronavirus cases,” but “everyone in the scientific and public health community expect it to be back in the fall and we expect to be in this for quite some time.” (Photo copyright: Texas A&M University.)
Marc Lipsitch, DPhil, Professor of Epidemiology and Director of the Center for Communicable Disease Dynamics at the Harvard T.H. Chan School of Public Health, is skeptical that warmer weather will put the brakes on COVID-19. “While we may expect modest declines in the contagiousness of SARS-CoV-2 in warmer, wetter weather, and perhaps with the closing of schools in temperate regions of the Northern Hemisphere, it is not reasonable to expect these declines alone to slow transmission enough to make a big dent,” he wrote in a commentary for the center.
How should pathologists and clinical laboratories in this country prepare for COVID-19? Lipsitch wrote that Influenza does tend to be seasonal, in part because cold, dry air is highly conducive to flu transmission. However, “for coronaviruses, the relevance of this factor is unknown.” And “new viruses have a temporary but important advantage—few or no individuals in the population are immune to them,” which means they are not as susceptible to the factors that constrain older viruses in warmer, more humid months.
So, we may not yet know enough to adequately prepare for
what’s coming. Nevertheless, monitoring the rapidly changing data on COVID-19
should be part of every lab’s daily agenda.