Occupancy rates at skilled nursing facilities remain well below pre-pandemic levels, a trend that weakens the financial health of nursing homes and means fewer test referrals to clinical laboratories that service them
COVID-19 is taking a financial bite out of the nursing home industry as seniors opt for home care rather than entering nursing facilities. If this trend becomes permanent, clinical laboratories may have to ramp up their ability to collect specimens from a growing population of patients who choose non-traditional healthcare settings. And as the SARS-CoV-2 pandemic stretches on, the exodus of seniors from nursing home facilities provides another example of how COVID-19 is altering consumers’ access to healthcare.
According to the most recent “AARP Nursing Home COVID-19 Dashboard Fact Sheets,” the COVID-19 pandemic “has swept the nation, killing more than 160,000 residents and staff of nursing homes and other long-term care facilities.”
Because COVID-19 has hit nursing home residents the hardest, many families have decided elderly parents may be safer living with relatives than in nursing homes that have proven vulnerable to widespread outbreaks. In addition, COVID-19-related lockdowns in skilled nursing facilities (SNFs) have provided families with additional motivation to choose home care for elderly relatives.
For example, in “Should You Bring Mom Home from Assisted Living During the Pandemic?” retired Seattle physician Alison Webb, MD, told Kaiser Health News (KHN) she moved her 81-year-old father, who has moderate dementia, out of assisted living so he could be with grandchildren and enjoy gardening rather than remain in his senior facility, where COVID-19 protocols kept him sequestered from friends and family.
This is not an isolated example and may have a long-term impact on clinical laboratories that service skilled nursing facilities.
Patient Volume Falls Dramatically at Skilled Nursing Facilities
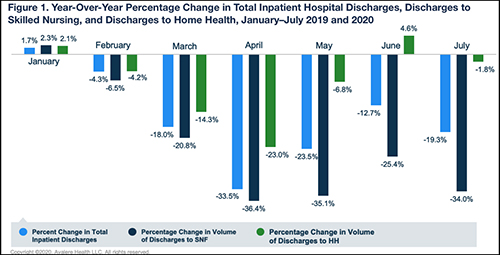
While hospital discharge rates are rebounding to near pre-pandemic levels, an Avalere Health analysis of Medicare fee-for-service claims found a “more drastic and lasting decline in patient volume” at skilled nursing facilities. In contrast, Avalere found home health has experienced a rebound in patient numbers beginning last May.
“In the early months of the COVID-19 outbreak in the US, we saw a substantial decrease in hospital discharges to both skilled nursing facilities and home health agencies,” said Heather Flynn, Consultant at Avalere, in an Avalere press release. “Hospital discharges are steadily moving back to pre-pandemic levels, but our analysis points to an uneven ‘return to normal’ across care settings.”
The graph above, taken from the Avalere press release, reveals “a stark decline in inpatient hospital discharges and discharges to both SNF and home health beginning in February 2020. The analysis further indicated that the skilled nursing industry has experienced a more drastic and lasting decline in patient volume relative to total hospital volume and discharges to home health (where rebounds were observed beginning in May). Of note, discharges to home health experienced a year-over-year increase in June 2020, at 4.6% greater discharge volume when compared to June 2019, while discharges to SNF remained notably below pre-pandemic levels at a 25.4% decrease in year-over-year discharges.” (Graphic copyright: Avalere Health.)
“Skilled nursing facility occupancy typically slows in April after an uptick during the flu season, but we haven’t seen anything like this in recent memory,” Kauffman said in an NIC press release which announced nursing home occupancy had dropped to 78.9% last April, 2020, down 5.5% from 2019. “The long-term effect of COVID-19 on skilled nursing occupancy remains to be seen as the industry adjusts to a new normal.”
Since then, the occupancy rate in skilled nursing properties has fallen even further. The latest Skilled Nursing Monthly Report announced a new low of 74.2%.
Will Clinical Laboratories That Service Skilled Nursing Homes Be Affected?
Mark Parkinson (above), President and CEO of the AHCA and former Governor of Kansas, maintains a successful COVID-19 vaccination rollout and lifting of nursing home visitation bans are keys to the industry’s recovery. “I think the census needs to recover about 1% a month. If we can recover 1% a month on a steady basis, that gets us to the end of 2021,” Parkinson told Skilled Nursing News. “And we’re still down, but we’re down 5% or 6%; we’re not down 13% or 14%. If we recover a half a percent, some businesses will be okay, but not all. If we only recover half a percent, we don’t get any more money, folks are going to have problems. If we don’t have any recovery on census … things are very, very bad.” (Photo copyright: Kansas Health Institute.)
There are signs the nursing home industry may have to contend with home healthcare becoming a permanent competitor for patients. In a news release last spring, the Mayo Clinic announced it was partnering with Medically Home of Boston to launch a virtual hospital-at-home model aimed at delivering “advanced care” from a network of paramedics, nurses, and support team in a home care setting.
The initiative means patients can receive a range of healthcare services in their homes that traditionally required a hospital setting. The services include:
Infusions,
Skilled nursing,
Clinical laboratory and imaging services,
Behavioral health and rehabilitation services.
While the initial program rollout will allow Mayo Clinic to free up ventilators and hospital space for COVID-19 patients, John Halamka, MD, an emergency medicine physician and President of Mayo Clinic Platform, told Modern Healthcare, “Next, we’ll look to forward-thinking organizations who believe like we do in that care should be more convenient and accessible.”
Discharge Doctors Now Choose Home Healthcare Over Skilled Nursing Facilities
Physicians also are embracing home care in greater numbers. As reported in Forbes, a 2020 William Blair survey showed 81% of physicians responsible for discharge planning would send patients to a home health agency rather than a skilled nursing facility. Pre-pandemic, only 54% of discharging physicians expressed a preference for home care, according to the survey.
Greg Chittim, Partner at Health Advances, an international strategy consulting firm headquartered in Boston, points to improvements in virtual technologies as the catalyst for home care’s growth.
“One of the silver linings of COVID-19 is the level of investment we are seeing in virtual care technologies,” Chittim told Forbes. “And beyond the technologies, providers and patients are building that comfort with traditional real-time communication. I think we have moved 10 years ahead in 10 months.”
As the COVID-19 pandemic rolls on and home health initiatives become more commonplace and grow in popularity, clinical laboratory managers may want to develop solutions that assist home healthcare providers with collecting and shipping patient specimens for testing.
With improved genetic sequencing comes larger human genome databases that could lead to new diagnostic and therapeutic biomarkers for clinical laboratories
As the COVID-19 pandemic grabbed headlines, the human genome database at the US Department of Veterans Affairs Million Veterans Program (MVP) quietly grew. Now, this wealth of genomic information—as well as data from other large-scale genomic and genetic collections—is expected to produce new biomarkers for clinical laboratory diagnostics and testing.
In December, cancer genomics company Personalis, Inc. (NASDAQ:PSNL) of Menlo Park, Calif., achieved a milestone and delivered its 100,000th whole human genome sequence to the MVP, according to a news release, which also states that Personalis is the sole sequencing provider to the MVP.
The VA’s MVP program, which started in 2011, has 850,000 enrolled veterans and is expected to eventually involve two million people. The VA’s aim is to explore the role genes, lifestyle, and military experience play in health and human illness, notes the VA’s MVP website.
Health conditions affecting veterans the MVP is researching include:
The VA has contracted with Personalis through September 2021, and has invested $175 million, Clinical OMICS reported. Personalis has earned approximately $14 million from the VA. That’s about 76% of the company’s revenue, according to 2nd quarter data, Clinical OMICS noted.
“The VA MVP is the largest whole genome sequencing project in the United States, and this is a significant milestone for both the program and for Personalis,” said John West (above with wife Judy), Founder and CEO of Personalis, in the news release. “Population-scale sequencing projects of this nature represent a cornerstone in our effort to accelerate the advancement of precision medicine across a wide range of disease areas,” he added. (Photo copyright: MIT Technology Review.)
Database of Veterans’ Genomes Used in Current Research
What has the VA gained from their investment so far? An MVP fact sheet states researchers are tapping MVP data for these and other veteran health-related studies:
Differentiating between prostate cancer tumors that require treatment and others that are slow-growing and not life-threatening.
How genetics drives obesity, diabetes, and heart disease.
How data in DNA translates into actual physiological changes within the body.
Gene variations and patients’ response to Warfarin.
NIH Research Program Studies Effects of Genetics on Health
Another research program, the National Institutes of Health’s All of Us study, recently began returning results to its participants who provided blood, urine, and/or saliva samples. The NIH aims to aid research into health outcomes influenced by genetics, environment, and lifestyle, explained a news release. The program, launched in 2018, has biological samples from more than 270,000 people with a goal of one million participants.
“We’re changing the paradigm for research. Participants are our most important partners in this effort, and we know many of them are eager to get their genetic results and learn about the science they’re making possible,” said Josh Denny, MD, CEO of the NIH’s All of Us research program in the news release. Denny, a physician scientist, was Professor of Biomedical Informatics and Medicine, Director of the Center for Precision Medicine and Vice President for Personalized Medicine at Vanderbilt University Medical Center prior to joining the NIH. (Photo copyright: National Institutes of Health.)
Inclusive Data Could Aid Precision Medicine
The news release notes that more than 80% of biological samples in the All of Us database come from people in communities that have been under-represented in biomedical research.
“We need programs like All of Us to build diverse datasets so that research findings ultimately benefit everyone,” said Brad Ozenberger, PhD, All of Us Genomics Program Director, in the news release.
Precision medicine designed for specific healthcare populations is a goal of the All of Us program.
“[All of Us is] beneficial to all Americans, but actually beneficial to the African American race because a lot of research and a lot of medicines that we are taking advantage of today, [African Americans] were not part of the research,” Chris Crawford, All of US Research Study Navigator, told the Birmingham Times. “As [the All of Us study] goes forward and we get a big diverse group of people, it will help as far as making medicine and treatment that will be more precise for us,” he added.
Large Databases Could Advance Care
Genome sequencing technology continues to improve. It is faster, less complicated, and cheaper to sequence a whole human genome than ever before. And the resulting sequence is more accurate.
Thus, as human genome sequencing databases grow, researchers are deriving useful scientific insights from the data. This is relevant for clinical laboratories because the new insights from studying bigger databases of genomic information will produce new diagnostic and therapeutic biomarkers that can be the basis for new clinical laboratory tests as well as useful diagnostic assays for anatomic pathologists.
As coronavirus pandemic emerged, the Minnesota reference laboratory surged its testing capacity from 2,600 to 20,000 samples per day in an effort to meet ever-increasing demand
Over the past several years, medical laboratory workforce shortages worldwide have challenged clinical laboratory managers to process increasing numbers of clinical laboratory tests with fewer staff. But that did not prepare them for the Herculean task of processing millions of tests each week! According to the CDC’s COVID Data Tracker, as of January 11, 2021, labs nationwide have processed 264,642,631 PCR tests since the start of the SARS-CoV-2 pandemic.
How were medical laboratories able to ramp up their processing capability so quickly? Here’s one example.
A Massive Undertaking at Mayo Clinic Laboratories
On March 12, 2020, Mayo Clinic Laboratories (Mayo) of Rochester, Minn., became one of the first hospital-affiliated reference labs in the country to develop a test for the SARS-CoV-2 coronavirus. At that time, the Minneapolis Star Tribune reported, Mayo was processing 200 to 300 COVID-19 tests/day. By late March through early April, 5,000 to 6,000 COVID-testing samples were arriving daily, but the lab’s capacity topped out at 2,600 samples/day. Today, however, Mayo Clinic Laboratories processes 20,000 samples each day.
How did the Mayo increase its capacity to meet unprecedented demand for COVID-19 testing? According to the Rochester Post Bulletin (Post Bulletin) the laboratory’s tenfold increase in testing capacity “required a massive undertaking of planning, hiring, construction, acquisition of equipment, and a lot of imagination and adaptation.”
The Post Bulletin reported that Mayo Clinic Laboratories started with one advantage—it already owned two automated Roche cobas SARS-CoV-2 systems that had received emergency-use authorization (EUA) from the FDA in March to test for the novel coronavirus.
But as demand for processing kits rose worldwide, the clinical laboratory could obtain only enough kits to process 4,500 tests per day, effectively limiting testing capacity to half, the Post Bulletin reported.
Mayo responded to the supply-chain disruptions by adding less-automated platforms to their testing arsenal. But using systems that required more manpower and took longer to process tests meant lab managers needed to hire even more staff.
During a two-week span in November, the laboratory added 180 new staff, four times the number of new hires in a typical year. To get new hires on the lab floor faster, a two-week orientation course was transformed into a condensed one-day training session. Other spots were filled by employees transferring in from other departments.
The photo above shows “Racks of COVID-19 test samples [being] unpacked and carted to available testing stations at the Rochester lab.” According to the Rochester Post Bulletin, “Mayo Clinic staff and volunteers handle tens of thousands of COVID-19 test samples daily from around the country at the Mayo Clinic Laboratories in Northwest Rochester.” (Photo and caption copyright: Rochester Post Bulletin/Ken Klotzbach.)
“It was kind of crazy. The size of the lab area just kept growing and growing,” said Ben Larson—who volunteered to move from his job as a lab processing assistant to a crew that processed COVID-19 samples in the Hepatitis/HIV Molecular Laboratory—in a Mayo Clinic Laboratories Insights blog post. “I thought it was cool, seeing all the COVID news and being able to say, ‘I’m actually working in the lab that’s doing the testing.’ It’s something I’ll tell my kids and grandkids. When there was the huge pandemic, I was working at Mayo Clinic as one of the people on the frontlines.”
Linda Spiten, Operations Administrator, Mayo Clinic Department of Laboratory Medicine and Pathology (DLMP), credits much of the lab’s success to the 400 DLMP staffers who shifted to different roles for the COVID transformation.
“We were definitely building the car as it was rolling down the street, because so much was hitting us so fast. But our staff is resilient and gracious. Knowing we didn’t have all the answers, but trusting, they took a leap of faith that we could work it out,” she said in the Insights blog post. “Many people made many sacrifices to work nights and weekends. We had people in labs working for weeks on end training in new folks, so we could make sure we had people ready to go. It was incredible.”
“A team of [clinical] technicians verify COVID-19 samples before passing it on for testing,” at Mayo Clinic Laboratories, Rochester Post Bulletin reported. (Photo and caption copyright: Rochester Post Bulletin/Ken Klotzbach.)
Clinical Laboratory Staff Shortages a Widespread Problem
Mayo Clinic Laboratories is not alone in facing supply-chain interruptions and staffing shortages during the pandemic. An Association for Molecular Pathology (AMP) survey in August of 2020 revealed the extent of the problem. More than 85% of respondents reported supply chain interruptions had delayed and/or decreased testing. The shortages most often cited were:
swabs (60%),
transport media (53%),
testing kits (34%),
reagents (33%),
testing platforms (32%).
Eighty-five percent of those surveyed said they have staffing shortages as well:
more than half (53%) reported not having enough medical technicians.
To manage these shortages, Mayo Clinic Laboratories found innovative ways to transform its operations. The Post Bulletin noted the lab implemented an employee’s suggestion to mark lab coats with color-coded duct tape, so that new hires could more easily identify supervisors’ roles and departments.
The need for added refrigeration was solved by parking 53-foot refrigerated trucks at the lab for storage of up to 15,000 pounds of dry ice each week, a changed that necessitated installing new doors on the building.
And according to the American Association of Clinical Chemistry (AACC), Mayo Clinic Laboratories also added a third shift to the workday to increase capacity and enable lab technologists to work spaced six feet apart.
“This management team has taught us to think on our feet,” lab worker Jane Masching told the Post Bulletin.
Infectious Disease Specialist Joseph Yao, MD, was tasked with coordinating the surge in Mayo Clinic’s testing capacity to 20,000 samples a day, an amount that still falls short of demand.
“I said we had better be prepared for the worst,” Yao told the Post Bulletin, noting the lab has received up to as many as 50,000 COVID test samples in a single day. “We’re still 15, 20 thousand behind. We’re always behind by about 24 hours.”
But some say there is reason to remain positive. Though the COVID-19 pandemic has clearly stretched clinical laboratories’ ingenuity, staffing, and workflow, Christopher Doern, PhD (above), Director of Clinical Microbiology at Virginia Commonwealth University School of Medicine in Richmond, Va., believes there is a silver lining for the clinical laboratory profession. He says the general public now has firsthand knowledge of the value of clinical laboratory medicine and its important role in patient care.
Nevertheless, while Mayo Clinic Laboratories is a prime example of how an organization can bring together the resources needed to meet the demand for COVID-19 tests, many clinical laboratories in the United States still struggle to hire more staff for the lab, as well as to obtain the needed volume of SARS-CoV-2 test kits and supplies.
Limited availability of COVID-19 clinical lab tests is major topic at federal briefings and news stories, yet many of nation’s labs are laying off staff and at point of closing
Cash flow at the nation’s clinical laboratories has crashed, with revenues down by more than $5 billion since early March. This is the biggest financial disaster for the nation’s clinical laboratory industry in its 100-year history and it couldn’t come at a worse time for the American public and the US healthcare system.
At the precise moment when the nation needs clinical laboratories to begin performing millions of tests for SARS-CoV-2, the coronavirus that causes the COVID-19 illness, those same labs are watching their cash flow collapse.
Data from multiple sources gathered by The Dark Report, sister publication of Dark Daily, confirm that—beginning in early March and continuing through last week—clinical laboratories in the United States saw incoming flows of routine specimens decline by between 50% and 60%. During this same time, lab revenue fell by similar amounts.
Clinical Lab Industry Currently Losing $800 to $900 Million Weekly
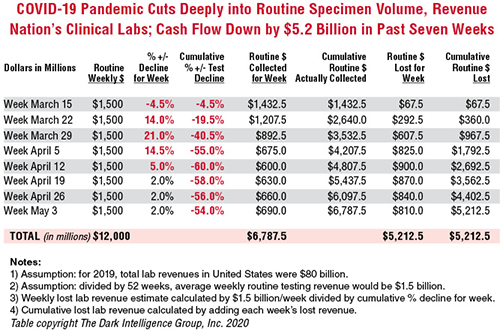
To give this decline context, the healthcare system spends about $80 billion annually on medical laboratory testing. Thus, labs across the US generated about $1.5 billion in revenue each week during 2019 and into 2020. By April 5, the decline in routine lab specimen volumes reached 55% to 60%. Since then, the clinical lab industry now loses between $800 million and $900 million each week. Total revenue loss from previous levels is already estimated to be $5.2 billion, and it is growing by an additional $800 million to $900 million every week that patients stay away from hospitals and physicians’ offices.
In the eight weeks since the COVID-19 pandemic caused patients to cease coming to hospitals and visiting their doctors, incoming routine specimens and revenue fell by 60%, causing cumulative lost routine revenue of $5.2 billion for the clinical laboratory industry in the United States. Each week that the existing shelter-in-place directives are effective, labs lose another $800 million to $900 million. The Dark Report based these estimates on data provided by multiple companies working with lab billing/claims, middleware analytical solutions, and customer relationship management (CRM) and electronic health record (EHR) products. (Chart copyright: The Dark Intelligence Group, Inc.)
The recent dire financial condition of labs small and large has gone unremarked by federal healthcare officials at the daily White House COVID-19 Task Force briefings. National news sources have yet to report on this development and its implications for successfully expanding the availability and numbers of COVID-19 tests in response to the pandemic.
The rapid and deep decline in specimens and revenue is not limited to clinical laboratories. Biopsy cases referred to anatomic pathology groups have declined by 50% to 60%. Some subspecialty pathology labs saw case referrals drop by 80% or more.
The nation’s two biggest clinical laboratory companies confirmed similar declines in their normal daily flow of routine specimens. Both companies recently reported first-quarter earnings (which included the month of March).
Quest Diagnostics, LabCorp Each Disclose Volume Declines of 50% to 60%
During its Q1 2020 earnings conference call, Chairman, President, and CEO of Quest Diagnostics (NYSE:DGX), Steve Rusckowski, stated, “In April, volume declines continue to intensify as we are seeing signs that volume declines are bottoming out at around 50% to 60%.”
The drop-off in routine lab test referrals was the similar at LabCorp (NYSE:LH). “In our diagnostics business, at the end of the quarter, we experienced reductions in demand for testing of 50% to 55% versus the company’s normal daily levels,” explained Glenn Eisenberg, Executive Vice President and CFO during LabCorp’s Q1 2020 earnings call. “This reduction in demand impacted testing volume broadly but was more heavily weighted towards routine procedures.”
Interviews with independent clinical lab owners and the administrative directors of hospital and health system labs further confirm this rapid and dramatic decline in the number of routine specimens arriving in their labs. Fewer specimens mean fewer claims, which means less revenue to laboratories.
Two Different Financial Futures for ‘Have’ Labs and ‘Have Not’ Labs
What happens next to the clinical laboratory industry in the United States—and to its ability to continue ramping up the availability of adequate numbers of COVID-19 tests in major cities, small towns, and rural areas—will be a story of “haves” and “have nots.”
The “haves” are clinical labs that have access to money. These are publicly-traded lab companies, academic medical center labs, and the sophisticated labs of health networks that operate multiple hospitals. In each case, these organizations have capital reserves and access to loans that will probably enable them to sustain COVID-19 lab testing services at the large volumes required to respond to the pandemic.
clinical labs operated by community hospitals and rural hospitals that were not financially robust before the onset of the pandemic; and,
specialty lab companies that perform a specific number of proprietary diagnostic tests (and for which demand has collapsed as patients stopped seeing their doctors).
Medicare Led Payers in the ‘Lab Test Price Race to the Bottom’
Prior to the onset of the SARS-CoV-2 pandemic, the finances of the “have-not” labs were already shaky, with many on the verge of filing bankruptcy, closing, or selling to a bigger lab company. Much blame for the deteriorating finances at a large proportion of community lab companies, community hospital labs, and rural hospital labs can be attributed to the deep, multi-year price cuts to the Medicare Part B clinical laboratory fee schedule as mandated by the Protecting Access to Medicare Act of 2014 (PAMA).
Medicare’s multi-year cuts to lab test prices were immediately copied by most state Medicaid programs. During this period, private payers followed Medicare’s lead and enacted their own deep cuts to the prices they paid labs for both routine tests and molecular/genetic tests.
That is why—when the pandemic intensified in early March—the 50% to 60% drop in specimens and revenue that hit these labs starved them of essential cash flow. When polled, the owners and directors of these labs acknowledge layoffs of the majority of their staff in all departments. They also reported substantial delays—both in submitted lab test claims and in getting payment for those claims—because claims-processing departments at the labs and private health insurers are understaffed due to shelter-in-place directives.
COVID-19 Test Revenue Helps Only Labs Performing Those Tests
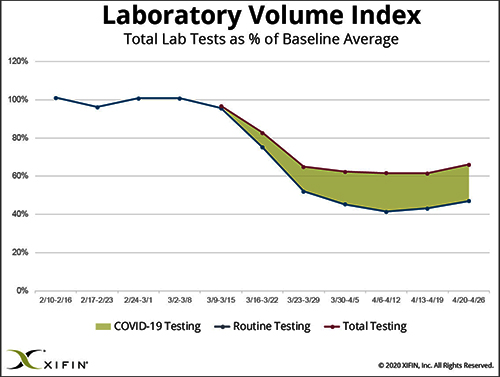
Revenue from COVID-19 testing is helping certain labs offset the revenue loss from fewer routine specimens. XIFIN, Inc., a San Diego company that provides revenue cycle management (RCM) services for clinical laboratories and pathology groups, analyzed the lab test claims for COVID-19 rapid molecular tests. It determined that labs performing these tests are generating enough revenue from these test claims to equal about 20% of their pre-pandemic revenue.
The chart above was prepared by XIFIN, Inc., of San Diego and is based on the changes XIFIN observed in the volume of routine clinical laboratory test claims generated by client labs on a weekly basis. In the first two months of 2020, routine lab test claims ran at expected levels until the first week of March. During the rest of March, routine lab test claims declined by 60%. During April, incoming routine lab test claims remained 55% to 60% below pre-pandemic levels. The shaded area shows the number of COVID-19 test claims coming into clinical labs. XIFIN says COVID-19 test claims make up about 20% of the decline in routine test specimens for those labs performing COVID-19 tests. The Dark Report estimates that the clinical laboratory industry has lost $800 million to $900 million in routine test revenue each week since March 23. Weekly revenue losses will continue at this rate until patients begin visiting their physicians and hospitals again perform elective services. (Chart copyright: XIFIN, Inc.)
Many CLIA-certified community laboratories and hospital labs have the diagnostic instruments and experience to perform rapid molecular tests for COVID-19. But when contacted, they tell us that their suppliers do not ship them even minimal quantities of the COVID-19 kits, the reagents, and the consumables. Thus, they cannot meet the needs of their client physicians. Instead, they watch as these physicians refer COVID-19 tests to the nation’s largest labs. The supply shortage prevents these smaller labs from doing larger numbers of COVID-19 test for the patients in the communities they serve. It also prevents them from earning the revenues from COVID-19 testing that currently helps the nation’s “have” labs offset the decline in revenue from routine testing.
Congress, national healthcare policymakers, and state governors need to immediately address this situation. Each week that passes during the COVID-19 pandemic and the shelter-in-place directives drains another $800 million to $900 million in revenue from routine lab testing that previously flowed into the nation’s clinical laboratories.
‘Have-not’ Clinical Labs in Small Towns Will Quietly Shrink and Disappear
Without timely intervention and financial support, the nation’s network of ‘have not’ labs, which have so capably served towns away from big metropolitan centers and rural areas, will quietly begin shrinking. One at a time, labs in small towns will close or sell. Local lab facilities will be shuttered and specimens from small-town patients will be transported to big labs hundreds or thousands of miles away.
It is also true that the financial disaster besetting the nation’s clinical laboratory industry will have comparable dramatic consequences for the in vitro diagnostics (IVD) manufacturers that sell them automation, analyzers, reagents, and other supplies. Since early March, IVD manufacturers watched as the pandemic caused orders for new instruments to collapse. During these same weeks, their clinical lab customers ceased ordering routine test kits at pre-pandemic levels. Dark Daily will cover the challenges confronting the IVD and other diagnostics industries in future e-briefings.
Announcing Free COVID-19 STAT Intelligence Briefings for Clinical Labs
With the COVID-19 pandemic creating chaos in nearly every aspect of healthcare, business, and society, clinical labs and their suppliers need timely intelligence and analysis about the innovations and successes achieved by their peers. This week, Dark Daily and The Dark Report are launching COVID-19 STAT Intelligence Briefings (Copy and paste this URL into your browser: https://www.covid19briefings.com). This comprehensive service is free and will cover four basic areas of needs for clinical laboratories as they ramp up COVID-19 testing:
Daily and weekly COVID-19 testing dashboards to guide every lab’s short-term planning;
Proven steps for labs to introduce and validate COVID-19 tests (both rapid molecular tests and serology tests);
Getting paid for COVID-19 testing to ensure every lab’s financial stability and clinical quality; and
Legal and regulatory updates for labs doing COVID19 tests to ensure full compliance.
Also, to help clinical laboratory leaders deal with the coming wave of COVID-19 serology tests, we are producing a free webinar led by James O. Westgard, PhD, FACB, and Sten Westgard, Director of Client Services and Technology, of Westgard QC, Inc.
Each week that the SARS-CoV-2 pandemic continues, and strict shelter-in-place directives are in place, the clinical laboratory industry loses another almost $900 million in revenue from lower volumes of routine testing. No industry can survive when its incoming revenue collapses by 50% to 60% for sustained periods of time.
Will Congress Recognize the Need for a Financial Rescue of ‘Have-not’ Labs?
Thus, it is incumbent on Congress, elected officials, and healthcare policymakers to recognize the financial consequences of the pandemic to the nation’s clinical laboratories. That is particularly true of the ‘have-not’ clinical labs. They do not have the same access to decisionmakers in government as billion-dollar lab companies.
And yet, these labs located in small communities and rural areas often are the only local labs that can do STAT testing in a couple of hours, and where clinical pathologists are personally familiar with local physicians and patients.
These “have-not” labs are vital healthcare resources. They should receive the help they need to get through this unprecedented crisis that is the COVID-19 pandemic.
It can take up to eight days after onset of symptoms for a person’s immune system to develop antibodies, so serological tests are not designed for diagnosing recent or active infections, stated a Mayo Clinic news story. However, Reuters reported that the availability of serological tests is “a potential game changer” because they could identify people who are immune even if they had no symptoms or only mild symptoms.
“Ultimately, this might help us figure out who can get the country back to normal,” Florian Krammer, PhD, told Reuters. Krammer’s lab at the Icahn School of Medicine at Mount Sinai in New York City has developed a serological test. “People who are immune could be the first people to go back to normal life and start everything up again,” he said.
However, some experts advise that the presence of antibodies is not necessarily a “get out of jail free” card when it comes to the coronavirus. “Infectious disease experts say immunity against COVID-19 may last for several months and perhaps a year or more based on their studies of other coronaviruses, including Severe Acute Respiratory Syndrome (SARS), which emerged in 2003,” reported Reuters. “But [the experts] caution that there is no way to know precisely how long immunity would last with COVID-19, and it may vary person to person.”
Additionally, it is also “uncertain whether antibodies would be sufficient protection if a person were to be re-exposed to the virus in very large amounts,” such as in an emergency room or ICU, Reuters reported.
Serological Survey Studies Get Underway Worldwide
Aside from detecting potential immunity, the World Health Organization (WHO) says serological tests could be useful for widespread disease surveillance and epidemiological research.
In the US, the Vitalant
Research Institute is leading several large serological survey or
“serosurvey” studies in which regional blood centers save samples of donated
blood for antibody testing, Science
reported.
Science also reported on a similar WHO initiative in which six countries will pool data from their own antibody studies. And in the Netherlands, blood banks have begun screening thousands of blood donations for presence of antibodies, Wired reported.
FDA Emergency Use Authorization
On March 16, the federal Food and Drug Administration (FDA) announced that it would allow commercial development and distribution of serological tests that “identify antibodies (e.g., IgM, IgG) to SARS-CoV-2 from clinical specimens” without an Emergency Use Authorization (EUA). The agency noted that these tests are “less complex than molecular tests” used to detect active infections, and that the policy change is limited to such testing in medical laboratories or by healthcare workers at the point-of-care. “This policy does not apply to at home testing,” the FDA reiterated.
“Serological tests can play a critical role in the fight against COVID-19 by helping healthcare professionals to identify individuals who have overcome an infection in the past and have developed an immune response,” said FDA Commissioner Stephen M. Hahn, MD (above with President Trump during a Coronavirus Task Force press briefing), in an April 7 press statement. “In the future, this may potentially be used to help determine—together with other clinical data—that such individuals are no longer susceptible to infection and can return to work. In addition, these test results can aid in determining who may donate a part of their blood called convalescent plasma, which may serve as a possible treatment for those who are seriously ill from COVID-19.” (Photo copyright: CNBC.)
FDA Issues First EUA for Rapid Diagnostic Test
Cellex Inc., based in Research Triangle Park, N.C., received the first EUA for its qSARS-CoV-2 serological test on April 1. As with other rapid diagnostic tests (RDTs) under development, the qSARS-CoV-2 test detects the presence of immunoglobulin M (IgM) and immunoglobulin G (IgG) antibodies in human blood. The biotechnology company’s RDT can be used to test serum, plasma, or whole-blood specimens, stated Cellex, and can produce results in 15 to 20 minutes.
The FDA has authorized use of the antibody test only by laboratories certified under CLIA to perform moderate and high complexity tests. Cellex has set up a COVID-19 website with information about the qSARS-CoV-2 test for clinical laboratories, patients, and healthcare providers.
Other Serological Tests Under Development
Mayo
Clinic Laboratories announced on April 13 that it is ramping up
availability of an internally-developed serological test. “Initial capacity
will be 8,000 tests per day performed at laboratory locations across Mayo Clinic,” stated the announcement.
“Testing will be performed 24 hours a day, and Mayo Clinic Laboratories is working
to ensure turnaround time is as close as possible to 24 hours after receipt of
the sample.”
Emory University in Atlanta announced on April 13 that it will begin deploying its own internally developed antibody test. Initially, testing will be limited to 300 people per day, comprised of Emory Healthcare patients, providers, and staff members. Eventually, testing will be “expanded significantly,” said Emory, with a goal of 5,000 tests per day by mid-June.
RDTs are typically qualitative, meaning they produce a
positive or negative result, stated the Center for Health Security. An ELISA
test “can be qualitative or quantitative,” noted the Center, but it can take
one to five hours to produce results.
A third type of serological test—the neutralization assay—involves infecting a patient’s blood with live coronavirus to determine if antibodies exist that can inhibit growth of the virus. The test takes three to five days in a level 3 biosafety laboratory to produce results. The Straits Times reported on one laboratory in Singapore that developed a neutralization assay to trace the source of COVID-19 infections that originated in Wuhan, China.
Serological testing is another important tool clinical
laboratories and epidemiologists can use to fight and ultimately defeat the
COVID-19 pandemic and is worth watching.