It can take up to eight days after onset of symptoms for a person’s immune system to develop antibodies, so serological tests are not designed for diagnosing recent or active infections, stated a Mayo Clinic news story. However, Reuters reported that the availability of serological tests is “a potential game changer” because they could identify people who are immune even if they had no symptoms or only mild symptoms.
“Ultimately, this might help us figure out who can get the country back to normal,” Florian Krammer, PhD, told Reuters. Krammer’s lab at the Icahn School of Medicine at Mount Sinai in New York City has developed a serological test. “People who are immune could be the first people to go back to normal life and start everything up again,” he said.
However, some experts advise that the presence of antibodies is not necessarily a “get out of jail free” card when it comes to the coronavirus. “Infectious disease experts say immunity against COVID-19 may last for several months and perhaps a year or more based on their studies of other coronaviruses, including Severe Acute Respiratory Syndrome (SARS), which emerged in 2003,” reported Reuters. “But [the experts] caution that there is no way to know precisely how long immunity would last with COVID-19, and it may vary person to person.”
Additionally, it is also “uncertain whether antibodies would be sufficient protection if a person were to be re-exposed to the virus in very large amounts,” such as in an emergency room or ICU, Reuters reported.
Serological Survey Studies Get Underway Worldwide
Aside from detecting potential immunity, the World Health Organization (WHO) says serological tests could be useful for widespread disease surveillance and epidemiological research.
In the US, the Vitalant
Research Institute is leading several large serological survey or
“serosurvey” studies in which regional blood centers save samples of donated
blood for antibody testing, Science
reported.
Science also reported on a similar WHO initiative in which six countries will pool data from their own antibody studies. And in the Netherlands, blood banks have begun screening thousands of blood donations for presence of antibodies, Wired reported.
FDA Emergency Use Authorization
On March 16, the federal Food and Drug Administration (FDA) announced that it would allow commercial development and distribution of serological tests that “identify antibodies (e.g., IgM, IgG) to SARS-CoV-2 from clinical specimens” without an Emergency Use Authorization (EUA). The agency noted that these tests are “less complex than molecular tests” used to detect active infections, and that the policy change is limited to such testing in medical laboratories or by healthcare workers at the point-of-care. “This policy does not apply to at home testing,” the FDA reiterated.
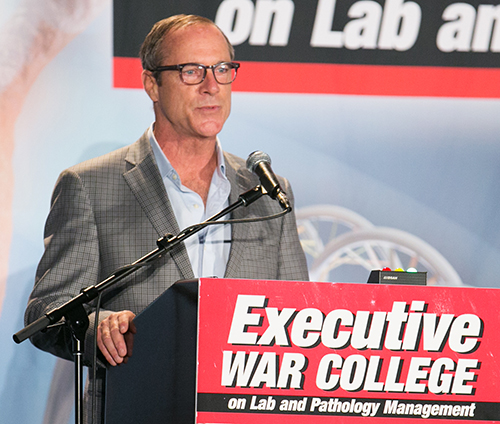
“Serological tests can play a critical role in the fight against COVID-19 by helping healthcare professionals to identify individuals who have overcome an infection in the past and have developed an immune response,” said FDA Commissioner Stephen M. Hahn, MD (above with President Trump during a Coronavirus Task Force press briefing), in an April 7 press statement. “In the future, this may potentially be used to help determine—together with other clinical data—that such individuals are no longer susceptible to infection and can return to work. In addition, these test results can aid in determining who may donate a part of their blood called convalescent plasma, which may serve as a possible treatment for those who are seriously ill from COVID-19.” (Photo copyright: CNBC.)
FDA Issues First EUA for Rapid Diagnostic Test
Cellex Inc., based in Research Triangle Park, N.C., received the first EUA for its qSARS-CoV-2 serological test on April 1. As with other rapid diagnostic tests (RDTs) under development, the qSARS-CoV-2 test detects the presence of immunoglobulin M (IgM) and immunoglobulin G (IgG) antibodies in human blood. The biotechnology company’s RDT can be used to test serum, plasma, or whole-blood specimens, stated Cellex, and can produce results in 15 to 20 minutes.
The FDA has authorized use of the antibody test only by laboratories certified under CLIA to perform moderate and high complexity tests. Cellex has set up a COVID-19 website with information about the qSARS-CoV-2 test for clinical laboratories, patients, and healthcare providers.
Other Serological Tests Under Development
Mayo
Clinic Laboratories announced on April 13 that it is ramping up
availability of an internally-developed serological test. “Initial capacity
will be 8,000 tests per day performed at laboratory locations across Mayo Clinic,” stated the announcement.
“Testing will be performed 24 hours a day, and Mayo Clinic Laboratories is working
to ensure turnaround time is as close as possible to 24 hours after receipt of
the sample.”
Emory University in Atlanta announced on April 13 that it will begin deploying its own internally developed antibody test. Initially, testing will be limited to 300 people per day, comprised of Emory Healthcare patients, providers, and staff members. Eventually, testing will be “expanded significantly,” said Emory, with a goal of 5,000 tests per day by mid-June.
RDTs are typically qualitative, meaning they produce a
positive or negative result, stated the Center for Health Security. An ELISA
test “can be qualitative or quantitative,” noted the Center, but it can take
one to five hours to produce results.
A third type of serological test—the neutralization assay—involves infecting a patient’s blood with live coronavirus to determine if antibodies exist that can inhibit growth of the virus. The test takes three to five days in a level 3 biosafety laboratory to produce results. The Straits Times reported on one laboratory in Singapore that developed a neutralization assay to trace the source of COVID-19 infections that originated in Wuhan, China.
Serological testing is another important tool clinical
laboratories and epidemiologists can use to fight and ultimately defeat the
COVID-19 pandemic and is worth watching.
Strategists agree that big tech is disrupting healthcare,
so how will clinical laboratories and anatomic pathology groups serve virtual
healthcare customers?
Visionary XPRIZE founder Peter Diamandis, MD, sees big tech as “the doctor of the future.” In an interview with Fast Company promoting his new book, “The Future Is Faster Than You Think,” Diamandis, who is the Executive Chairman of the XPRIZE Foundation, said that the healthcare industry is “phenomenally broken” and that Apple, Amazon, and Google could do “a thousandfold” better job.
Diamandis, who also founded Singularity University, a global learning and innovation community that uses exponential technologies to tackle worldwide challenges, according to its website, said, “We’re going to see Apple and Amazon and Google and all the data-driven companies that are in our homes right now become our healthcare providers.”
If this prediction becomes reality, it will bring significant changes in the traditional ways that consumers and patients have selected providers and access healthcare services. In turn, this will require all clinical laboratories and pathology groups to develop business strategies in response to these developments.
Amazon Arrives in Healthcare Markets
Several widely-publicized business initiatives by Amazon, Google, and Apple substantiate these predictions. According to an Amazon blog, healthcare insurers, providers, and pharmacy benefit managers are already operating HIPAA-eligible Amazon Alexa for:
Alexa also enables HIPAA-compliant blood glucose updates as part of the Livongo for Diabetes program. “Our members now have the ability to hear their last blood glucose check by simply asking Alexa,” said Jennifer Schneider, MD, President of Livongo, a digital health company, in a news release.
And Cigna’s “Answers By Cigna” Alexa “skill” gives members who install the option responses to 150 commonly asked health insurance questions, explained a Cigna news release.
“Google plans to disrupt healthcare and use data and artificial intelligence,” Toby Cosgrove, Executive Advisor to the Google Cloud team and former Cleveland Clinic President, told B2B information platform PYMNTs.com.
PYMNTs speculated that Google, which recently acquired Fitbit, could be aiming at connecting consumers’ Fitbit fitness watch data with their electronic health records (EHRs).
“Ultimately what’s best is human and AI collaboratively,” Peter Diamandis, MD, founder of XPRIZE Foundation and Singularity University told Fast Company. “But I think for reading x-rays, MRIs, CT scans, genome data, and so forth, that once we put human ego aside, machine learning is a much better way to do that.” (Photo copyright: SALT.)
Apple Works with Insurers, Integrating Health Data
The Apple Watch health app also enables people to access medical laboratory test results and vaccination records, and “sync up” information with some hospitals, Business Insider explained.
Virtual Care, a Payer Priority: Survey
Should healthcare providers feel threatened by the tech giants? Not necessarily. However, employers and payers surveyed by the National Business Group on Health (NBGH), an employer advocacy organization, said they want to see more virtual care solutions, a news release stated.
“One of the challenges employers face in managing their healthcare costs is that healthcare is delivered locally, and change is not scalable. It’s a market-by-market effort,” said Brian Marcotte, President and CEO of the NBGH, in the news release. “Employers are turning to market-specific solutions to drive meaningful changes in the healthcare delivery system.
“Virtual care solutions bring healthcare to the consumer
rather than the consumer to healthcare,” Marcotte continue. “They continue to
gain momentum as employers seek different ways to deliver cost effective,
quality healthcare while improving access and the consumer experience.”
“In AI, there are three trends to watch,” said health strategist Ted Schwab (above) while speaking at the 2019 Executive War College. “The first major AI trend will affect clinical laboratories and pathologists. It involves how diagnosis will be done on the Internet and via telehealth. The second AI trend is care delivery, such as what we’ve seen with Amazon’s Alexa—you should know that Amazon’s business strategy is to disrupt healthcare. And the third AI trend involves biological engineering,” he concluded. (Photo copyright: Dark Daily.)
“If you use Google in the United States to check symptoms,
you’ll get five-million to 11-million hits,” Schwab told The Dark Report.
“Clearly, there’s plenty of talk about symptom checkers, and if you go online
now, you’ll find 350 different electronic applications that will give you
medical advice—meaning you’ll get a diagnosis over the internet. These
applications are winding their way somewhere through the regulatory process.
“The FDA just released a report saying it plans to regulate
internet doctors, not telehealth doctors and not virtual doctors,” he
continued. “Instead, they’re going to regulate machines. This news is
significant because, today, within an hour of receiving emergency care, 45% of
Americans have googled their condition, so the cat is out of the bag as it
pertains to us going online for our medical care.”
Be Proactive, Not Reactive, Health Leaders Say
Healthcare leaders need to work on improving access to primary care, instead of becoming defensive or reactive to tech companies, several healthcare CEOs told Becker’s Hospital Review.
Clinical laboratory leaders are advised to keep an eye on
these virtual healthcare trends and be open to assisting doctors engaged in
telehealth services and online diagnostic activities.
By offering DTC preventative gene sequencing, hospital leaders
hope to help physicians better predict cancer risk and provide more accurate
diagnoses
Two Boston health systems, Brigham and Women’s Hospital and Massachusetts General Hospital (MGH), are the latest to open preventative gene sequencing clinics and compete with consumer gene sequencing companies, such as 23andMe and Ancestry, as well as with other hospital systems that already provide similar services.
This may provide opportunities for clinical laboratories. However, some experts are concerned that genetic sequencing may not be equally available to patients of all socioeconomic classes. Nor is it clear how health systems plan to pay for the equipment and services, since health insurance companies continue to deny coverage for “elective” gene sequencing, or when there is not a “clear medical reason for it, such as for people with a long family history of cancer,” notes STAT.
Therefore, not everyone is convinced of the value of gene sequencing to either patients or hospitals, even though advocates tout gene sequencing as a key element of precision medicine.
Is Preventative Genetic Sequencing Ready for the Masses?
Brigham’s Preventive Genomics Clinic offers comprehensive DNA sequencing, interpretation, and risk reporting to both adults and children. And MGH “plans to launch its own clinic for adults that will offer elective sequencing at a similar price range as the Brigham,” STAT reported.
The Brigham and MGH already offer similar gene sequencing services as other large health systems, such as Mayo Clinic and University of California San Francisco (UCSF), which are primarily used for research and cancer diagnoses and range in price depending on the depth of the scan, interpretation of the results, and storage options.
However, some experts question whether offering the
technology to consumers for preventative purposes will benefit anyone other
than a small percentage of patients.
“It’s clearly not been demonstrated to be cost-effective to promote this on a societal basis,” Robert Green, MD, MPH, medical geneticist at Brigham and Women’s Hospital, and professor of genetics at Harvard, told STAT. “The question that’s hard to answer is whether there are long-term benefits that justify those healthcare costs—whether the sequencing itself, the physician visit, and any downstream testing that’s stimulated will be justified by the situations where you can find and prevent disease.”
Additionally, large medical centers typically charge more
for genomic scans than consumer companies such as 23andMe and Ancestry. Hospital-based
sequencing may be out of the reach of many consumers, and this concerns some
experts.
“The idea that genomic sequencing is only going to be
accessible by wealthy, well-educated patrons who can pay out of pocket is
anathema to the goals of the publicly funded Human Genome Project,” Jonathan
Berg, MD, PhD, Genetics Professor, University of North Carolina at Chapel
Hill, told Scientific
American.
And, according to the American Journal of Managed Care, “It’s estimated that by 2021, 100 million people will have used a direct-to-consumer (DTC) genetic test. As these tests continue to gain popularity, there is a need for educating consumers on their DTC testing results and validating these results with confirmatory testing in a medical-grade laboratory.”
This is why it’s critical that clinical laboratories and
anatomic pathology groups have a genetic testing and gene sequencing strategy,
as Dark
Daily reported.
David Bick, MD, Chief Medical Officer at the HudsonAlpha Institute for Biotechnology and Medical Director of the Smith Family Clinic for Genomic Medicine, told Scientific American, “there’s just more and more interest from patients and families not only because of 23andMe and the like, but because there’s just this understanding that if you can find out information about your health before you become sick, then really our opportunity as physicians to do something to help you is much greater.”
In an article he penned for Medium, Robert Green, MD, MPH (shown above counseling a patient), medical geneticist at Brigham and Women’s Hospital and professor of genetics at Harvard, wrote, “The ultimate aim of our Genomes2People Research Program is to contribute to the transformation of medicine from reactive to proactive, from treatment-oriented to preventive. We are trying to help build the evidence base that will justify societal decision to make these technologies and services accessible to anyone who wants them, regardless of means, education or race and ethnicity.” (Photo copyright: Wall Street Journal.)
Is Preventative Genomics Elitist?
As large medical centers penetrate the consumer genetic
testing market some experts express concerns. In a paper he wrote for Medium,
titled, “Is Preventive Genomics Elitist?” Green asked, “Is a service like this
further widening the inequities in our healthcare system?”
Green reported that while building the Preventive Genomics Clinic at Brigham, “we … struggled with the reality that there is no health insurance coverage for preventive genomic testing, and our patients must therefore pay out of pocket. This is a troubling feature for a clinic at Brigham and Women’s Hospital, which is known for its ties to communities in Boston with diverse ethnic and socioeconomic backgrounds.”
Most of Brigham’s early genetics patients would likely be “well-off,
well-educated, and largely white,” Green wrote. “This represents the profile of
typical early adopters in genetic medicine, and in technology writ large. It
does not, however, represent the Clinic’s ultimate target audience.”
More Data for Clinical Laboratories
Nevertheless, preventive genomics programs offered by large
health systems will likely grow as primary care doctors and others see evidence
of value.
Therefore, medical laboratories that process genetic
sequencing data may soon be working with growing data sets as more people reach
out to healthcare systems for comprehensive DNA sequencing and reporting.
Number of patients eligible for genome-driven oncology therapy is increasing, but the percentage who reportedly benefit from the therapy remains at less than 5%
Advances in precision medicine in oncology (precision oncology) are fueling the need for clinical laboratory companion diagnostic tests that help physicians choose the best treatment protocols. In fact, this is a fast-growing area of clinical diagnostics for the nation’s anatomic pathologists. However, some experts in the field of genome-based cancer treatments disagree over whether such treatments offer more hype than hope.
Prasad and his colleagues evaluated 31 US Food and Drug
Administration (FDA) approved drugs, which were “genome-targeted” or
“genome-informed” for 38 indications between 2006 and 2018. The researchers
sought to answer the question, “How many US patients with cancer are eligible
for and benefit annually from genome-targeted therapies approved by the US Food
and Drug Administration?”
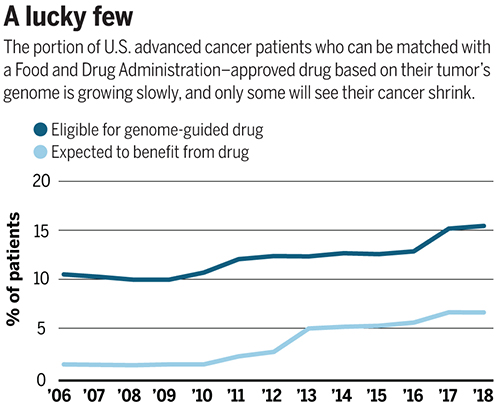
They found that in 2018 only 8.33% of 609,640 patients with
metastatic cancer were eligible for genome-targeted therapy—though this was an
increase from 5.09% in 2006.
Even more telling from Prasad’s view, his research team concluded
that only 4.9% had benefited from such treatments. Prasad’s study found the
percentage of patients estimated to have benefited from genome-informed therapy
rose from 1.3% in 2006 to 6.62% in 2018.
“Although the number of patients eligible for genome-driven treatment has increased over time, these drugs have helped a minority of patients with advanced cancer,” the researchers concluded. “To accelerate progress in precision oncology, novel trial designs of genomic therapies should be developed, and broad portfolios of drug development, including immunotherapeutic and cytotoxic approaches, should be pursued.”
The graph above is based on data from a study published in Science titled, “Estimation of the Percentage of US Patients With Cancer Who Benefit from Genome-Driven Oncology,” co-authored by Vinay Prasad, MD, MPH, et al. (Image copyright: Science.)
A Value versus Volume Argument?
Hyman, who leads a team of oncologists that conduct dozens
of clinical trials and molecularly selected “basket studies” each year,
countered Prasad’s assertions by noting the increase in the number of patients
who qualify for precision oncology treatments.
As reported in Science, Hyman said during his AACR
presentation that Sloan Kettering matched 15% of the 25,000 patients’ tumors it
tested with FDA-approved drugs and 10% with drugs in clinical trials.
“I think this is certainly not hype,” he said during the
conference.
Hyman added that another 10% to 15% of patient tumors have a
DNA change that matches a potential drug tested in animals. He expects “basket”
trials to further increase the patient pool by identifying drugs that can work
for multiple tumor types.
The US National Institute of Health (NIH) describes “basket studies” as “a new sort of clinical studies to identify patients with the same kind of mutations and treat them with the same drug, irrespective of their specific cancer type. In basket studies, depending on the mutation types, patients are classified into ‘baskets.’ Targeted therapies that block that mutation are then identified and assigned to baskets where patients are treated accordingly.”
Are Expectations of Precision Medicine Exaggerated?
A profile in MIT Technology Review, titled, “The Skeptic: What Precision Medicine Revolution?,” describes Prasad’s reputation as a “professional scold” noting the 36-year-old professor’s “sharp critiques of contemporary biomedical research, including personalized medicine.” Nevertheless, Prasad is not alone in arguing that precision oncology’s promise is often exaggerated.
“Like most ‘moonshot’ medical research initiatives,
precision medicine is likely to fall short of expectations,” Joyner wrote.
“Medical problems and their underlying biology are not linear engineering
exercises and solving them is more than a matter of vision, money, and will.”
“Although some niche applications have been found for
precision medicine—and gene therapy is now becoming a reality for a few rare
diseases—the effects on public health are miniscule while the costs are astronomical,”
they wrote.
Hope for Precision Medicine Remains High
However, optimism over precision oncology among some industry leaders has not waned. Cindy Perettie, CEO of molecular information company Foundation Medicine of Cambridge, Mass., argues genome-directed treatments have reached an “inflection point.”
“Personalized cancer treatment is a possibility for more patients than ever thanks to the advent of targeted therapies,” she told Genetic Engineering and Biotechnology News. “With a growing number of new treatments—including two pan-tumor approvals—the need for broad molecular diagnostic tools to match patients with these therapies has never been greater. We continue to advance our understanding of cancer as a disease of the genome—one in which treatment decisions can be informed by insight into the genomic changes that contribute to each patient’s unique cancer.”
Prasad acknowledges genome-driven therapies are beneficial for some cancers. However, he told MIT Technology Review the data doesn’t support the “rhetoric that we’re reaching exponential growth, or that is taking off, or there’s an inflection point” signaling rapid new advancements.
“Right now, we are investing heavily in immunotherapy and heavily in genomic therapy, but in other categories of drugs, such as cytotoxic drugs, we have stopped investigating in them,” he told Medscape Medical News. “But it’s foolish to do this—we need to have the vision to look beyond the fads we live by in cancer medicine and do things in a broader way,” he added.
“So, I support broader funding because you have to sustain
efforts even when things are not in vogue if you want to make progress,” Prasad
concluded.
Is precision oncology a fad? Dark Daily has covered the advancements in precision medicine extensively over the past decade, and with the launch of our new Precision Medicine Institute website, we plan to continue reporting on further advancements in personalized medicine.
Time will tell if precision oncology can fulfill its
promise. If it does, anatomic pathologists will play an important role in
pinpointing patients most likely to benefit from genome-driven treatments.
One thing that the debate between proponents of precision
medicine in oncology and their critics makes clear is that more and better
clinical studies are needed to document the true effectiveness of target
therapies for oncology patients. Such evidence will only reinforce the
essential role that anatomic pathologists play in diagnosis, guiding
therapeutic decisions, and monitoring the progress of cancer patients.
Some companies save so much in healthcare cost they pay their employees to participate in medical tourism programs
Medical tourism is not new, but it’s changing, and clinical laboratories have a role to play in the models employers use to save money on their employees’ health coverage costs.
Employers that manage the entire process—from securing
passports for their employees, to ensuring they have access to high-quality care
outside the country’s borders—report saving money as well as simplifying the
process for their employees. An apparent win-win.
However, questions linger about:
Availability of diagnostic testing and clinical
laboratories;
If patients treated outside the US receive
adequate protections; and
Whether the quality of care is equal to that in
the US.
One recent example of a company helping employers and employees receive high quality care outside of the US is NASH—the North American Specialty Hospital. NASH was featured in a Kaiser Health News (KHN) article that described one patient’s experience traveling to Cancún for a surgical procedure.
Location, Pre-Existing Conditions, Length of Stay, Etc.,
Affect Final Bill in US
One of NASH’s corporate clients is Ashley Furniture Industries. Headquartered
in Arcadia, Wis., the American home furnishings manufacturer and retailer employs
approximately 17,000 people, including Terry Ferguson. Terry’s wife, Donna, is
the patient highlighted in the KHN story.
One of the healthcare providers NASH partners with is Galenia Hospital, a 55-bed general services hospital in Cancún, Mexico. NASH leases the entire third floor of the hospital. Galenia is next door to a Four Points Sheraton Hotel, making lodging a simple matter for medical tourists.
Currently, NASH focuses on orthopedic surgeries such as total
knee replacements, the medical procedure Donna Ferguson underwent.
A 2015 BlueCross
BlueShield study showed that costs for total-knee-replacement surgery in
the US averaged about $31,000. However, depending on where the surgery takes
place, it can cost as low as $11,317 (Alabama) and as high as $69,654 (New York
City). Pre-existing conditions, length of time in the operating room, number of
days in the hospital, and numerous other factors contribute to the final bill.
NASH, however, sets the final price is up front.
Some Companies Pay Their Employees to Use Medical Tourism
With the average cost for the surgery coming in at around
$12,000, the cost savings to employers is so great some companies actually pay employees
who are willing to travel for procedures, KHN reported. Donna Ferguson paid
no co-pays for her surgery, paid nothing out of pocket for travel or lodging
while in Cancún, and the Ferguson’s received a $5,000 check from Ashley
Furniture.
Ferguson told KHN, “It’s been a great experience.
Even if I had to pay, I would come back here because it’s just a different
level of care—they treat you like family.”
That’s important for hospitals, clinical laboratories, and
all healthcare providers in America to consider. In the minds of patients,
quality of care starts with their experience at the hands of the provider.
Donna Ferguson (center) is shown above meeting Thomas Parisi, MD, JD (left), a surgeon with the Orthopedic Institute of Wisconsin, for the first time in Cancún the day before he performed her knee replacement surgery. Clinical laboratory tests, X-rays, and other diagnostics took place in the US prior to Ferguson’s authorization to undergo surgery in Mexico. (Photo copyright: Rocco Saint-Mleux/KHN.)
Clinical Laboratory Tests in US, Surgery in Mexico
Prior to traveling outside the US for surgery, Ferguson
underwent a physical exam, X-rays, and other diagnostic testing to ensure the
treatment approach was the best for her. Once that was confirmed, IndusHealth, Ashely’s medical travel
plan administrator, “coordinated [Donna’s] medical care and made travel
arrangements, including obtaining passports, airline tickets, hotel and meals,”
for both Donna and Terry Ferguson, KHN reported.
It seems reasonable to assume that NASH has agreements with
multiple clinical pathology laboratories and healthcare facilities throughout
the US for patients to get the tests they need prior to surgery. Partnerships
with medical tourism companies may well represent an avenue for pathology
laboratories to pursue.
Protections for Patients
So, why hasn’t medical tourism become the healthcare juggernaut some experts predicted? Managed Care suggests one reason is that Americans tend to be skeptical of the quality of care they will receive in a foreign facility.
“Building a familiar culture in a foreign destination may be appealing to some American consumers, but I do not see it as a sustainable business,” Health consultant Irving Stackpole, PhD, MEd, Psychology, told KHN. “It’s not unusual for people thinking about this to have doctors, family, and friends who will see this as a high-risk undertaking.”
Several factors helped Ferguson feel better about her
decision to travel to Mexico for surgery. One is that Galenia is credentialed.
Managed Care notes, “A number of organizations credential international facilities. The American Medical Association guidelines for medical tourism recommend that foreign medical providers have accreditation from the Joint Commission International or a similar organization.”
In addition to a credentialed facility and a highly trained
surgeon, NASH also provides US malpractice insurance coverage, giving patients
recourse in the event something goes wrong. Ferguson and American patients like
her would be able to sue in the US if care under this arrangement was not
successful.
Medical Tourism Pays Surgeon’s Full Fee
One fascinating twist in this story is that an American physician was flown to Cancun to perform this operation and was paid his full fee. The surgeon scheduled to perform Ferguson’s operation, Thomas Parisi, MD, JD, trained at the Mayo Clinic. He traveled from Wisconsin to Cancún to perform the procedure. “Dr. Parisi trained at Mayo, and you can’t do any better than that,” Ferguson told KHN.
KHN reported that Parisi spent less than 24 hours in
Cancun and was paid $2,700 for this surgery. That fee is three times of the
amount Medicare pays for this procedure. Further, Parisi’s fee was
significantly above what many managed care plans would negotiate for this type
of surgery.
American-trained physicians are common at many of the
facilities credentialed by the Joint Commission International. “Many overseas
hospitals are staffed in part by physicians and other health professionals who
were trained in US hospitals. One hospital in India has 200 US-trained
board-certified surgeons,” wrote James E. Dalen, MD,
MPH, ScD, and Joseph S. Alpert,
MD, in “Medical Tourists: Incoming and Outgoing,” published in The American
Journal of Medicine (AMJMED).
“In the past, medical tourism has been mostly a blind leap to a country far away, to unknown hospitals and unknown doctors with unknown supplies, to a place without US medical malpractice insurance. We are making the experience completely different and removing as much uncertainty as we can,” James Polsfut, CEO and Chairman, North American Specialty Hospital (NASH), told KHN.
Clinical laboratories in America may find opportunities
providing testing services to medical tourism organizations like NASH. It’s
worth investigating.