Research in the UK and US into how rapid WGS can prevent deaths and improve outcomes for kids with rare genetic diseases may lead to more genetic testing based in local clinical laboratories
Genetic scientists with the National Health Service (NHS) in England have embarked on an ambitious plan to offer rapid whole genome sequencing (rWGS) for children and babies with serious illnesses, as part of a larger initiative to embrace genomic medicine in the United Kingdom (UK).
The NHS estimates that the plan will benefit more than 1,000 children and babies each year, including newborns with rare diseases such as cancer, as well as kids placed in intensive care after being admitted to hospitals. Instead of waiting weeks for results from conventional tests, clinicians will be able to administer a simple blood test and get results within days, the NHS said in a press release.
The press release notes that about 75% of rare genetic diseases appear during childhood “and are responsible for almost a third of neonatal intensive care deaths.”
Here in the United States, pathologists and clinical laboratory managers should see this development as a progressive step toward expanding access to genetic tests and whole genome sequencing services. The UK is looking at this service as a nationwide service. By contrast, given the size of the population and geography of the United States, as this line of medical laboratory testing expands in the US, it will probably be centered in select regional centers of excellence.
“This strategy sets out how more people will be empowered to take preventative action following risk-based predictions, receive life-changing diagnoses, and get the support needed to live with genomically-informed diagnoses alongside improved access to cutting-edge precision [medicine] treatments. It also outlines how the NHS will accelerate future high-quality genomic innovation that can be adopted and spread across the country, leading to positive impacts for current and future generations,” the NHS wrote.
“This global first is an incredible moment for the NHS and will be revolutionary in helping us to rapidly diagnose the illnesses of thousands of seriously ill children and babies—saving countless lives in the years to come,” said NHS chief executive Amanda Pritchard (above) in a press release announcing the program. (Photo copyright: Hospital Times.)
New Rapid Whole Genome Sequencing Service
The NHS announced the plan following a series of trials last year. In one trial, a five-day old infant was admitted to a hospital in Cheltenham, Gloucester, with potentially deadly levels of ammonia in his blood. Whole genome sequencing revealed that changes in the CPS1 gene were preventing his body from breaking down nitrogen, which led to the spike in ammonia. He was given life-saving medication in advance of a liver transplant that doctors believed would cure the condition. Without the rapid genetic test, doctors likely would have performed an invasive liver biopsy.
Using a simple blood test, the new newborn genetic screening service in England is expected to benefit more than 1,000 critically ill infants each year, potentially saving their lives. “The rapid whole genome testing service will transform how rare genetic conditions are diagnosed,” explained Emma Baple, PhD, Professor of Genomic Medicine at University of Exeter Medical School and leader of the National Rapid Whole Genome Sequencing Service in the press release. “We know that with prompt and accurate diagnosis, conditions could be cured or better managed with the right clinical care, which would be life-altering—and potentially life-saving—for so many seriously unwell babies and children,” Precision Medicine Institute reported.
According to The Guardian, test results will be available in two to seven days.
Along with the new rWGS testing service, the NHS announced a five-year plan to implement genomic medicine more broadly. The provisions include establishment of an ethics advisory board, more training for NHS personnel, and an expansion of genomic testing within the existing NHS diagnostic infrastructure. The latter could include using NHS Community Diagnostics centers to collect blood samples from family members to test for inherited diseases.
UK’s Longtime Interest in Whole Genome Sequencing
The UK government has long been interested in the potential role of WGS for delivering better outcomes for patients with genetic diseases, The Guardian reported.
In 2013, the government launched the 100,000 Genomes Project to examine the usefulness of the technology. In November 2021, investigators with the project reported the results of a large pilot study in which they analyzed the genomes of 4,660 individuals with rare diseases. The study, published in the New England Journal of Medicine (NEJM) titled, “100,000 Genomes Pilot on Rare-Disease Diagnosis in Health Care—Preliminary Report,” found “a substantial increase in yield of genomic diagnoses made in patients with the use of genome sequencing across a broad spectrum of rare disease.”
The study’s findings suggest that use of WGS “could save the NHS millions of pounds,” The Guardian reported.
Whole Genome Sequencing System for Newborns in the US
“This NBS-rWGS [newborn screening by rapid whole genome sequencing] system is designed to complement the existing newborn screening process and has the potential to eliminate the diagnostic and therapeutic odyssey that many children and parents face,” Kingsmore said in a press release. “Currently, only 35 core genetic disorders are recommended for newborn screening in the United States, but there are more than 7,200 known genetic diseases. Outcomes remain poor for newborns with a genetic disease because of the limited number of recommended screenings. With NBS-rWGS, we can more quickly expand that number and therefore potentially improve outcomes through precision medicine.”
A more recent 2023 study which examined 112 infant deaths at Rady Children’s Hospital found that 40% of the babies had genetic diseases. In seven infants, genetic diseases were identified post-mortem, and in five of them “death might have been avoided had rapid, diagnostic WGS been performed at time of symptom onset or regional intensive care unit admission,” the authors wrote.
“Prior etiologic studies of infant mortality are generally retrospective, based on electronic health record and death certificate review, and without genome information, leading to underdiagnosis of genetic diseases,” said Christina Chambers, PhD, co-author of the study, in a press release. “In fact, prior studies show at least 30% of death certificates have inaccuracies. By implementing broad use of genome sequencing in newborns we might substantially reduce infant mortality.”
Pioneering work with whole genome sequencing for newborns, such as that being conducted by the clinical laboratory and genetic teams at Rady Children’s Hospital and the UK’s NHS, could allow doctors to make timely interventions for our most vulnerable patients.
Under-resourced British healthcare system faces a record high backlog of care with 5.61 million people in England waiting for hospital-based medical procedures
Healthcare in the United Kingdom (UK) is about to become much more expensive. The UK government has announced plans to substantially increase payroll taxes to fund the surging demand for care due to the COVID-19 pandemic. But that may only be the part of the healthcare-funding iceberg visible above the surface. Below the surface is a healthcare system where wait times for access to many types of care—including cancer diagnoses—are already unacceptable.
Some pathologists and medical laboratory executives in the US who have long questioned healthcare reformers’ desire to introduce an NHS-like single-payer healthcare system in this country will not be surprised to learn that the UK’s notoriously underfunded National Health Service (NHS) is facing a record waitlist for hospital-based medical diagnostic tests and procedures.
Consequently, Reuters reported, the high cost of fighting the COVID-19 pandemic has pushed British Prime Minister Boris Johnson into breaking with election promises and announcing plans to raise payroll taxes to record levels so that more money can be funneled into the struggling government-run healthcare system.
Speaking to lawmakers in the House of Commons, British Prime Minister Boris Johnson (above) acknowledged his tax plan breaks his Conservative Party’s election year pledge to not raise VAT (value-added tax), income, or national insurance taxes. He insists that the COVID-19 pandemic created unprecedented challenges for the national health system. “I accept that this breaks a manifesto commitment, which is not something I do lightly, but a global pandemic was in no one’s manifesto,” he told lawmakers, Reuters reported. (Photo copyright: The Independent.)
5.6M People on Growing NHS Waiting List for Treatments and Procedures
When the COVID-19 pandemic struck the UK in March 2020, the NHS suspended elective surgeries such as hip or knee replacements and cataract removal and postponed many patients’ medical laboratory diagnostic tests.
In “Record 5.6M People in England Waiting for Hospital Treatment,” The Guardian estimated that 1.4 million patients were added to the waiting lists during the pandemic’s first 18 months. More than one-third of the 5.6 million people waiting for care in July 2021 had been on a waitlist for at least 18 months, the paper noted. Since then, the waiting list has grown by 150,000 people per month, as more people who did not seek or could not access NHS treatments during the pandemic returned to their doctors’ offices.
Johnson’s tax hike formula for fixing the record NHS backlog and improving social care for the elderly created shockwaves in the UK’s Conservative Party, which, like the Republican Party in this country, has championed low taxes. But Johnson maintains the government is out of options.
“It would be wrong for me to say that we can pay for this recovery without taking the difficult but responsible decisions about how we finance it,” Johnson told Parliament. “It would be irresponsible to meet the costs from higher borrowing and higher debt,” he added.
But Johnson’s proposal drew the wrath of some members of his own party and provided the opposition Labor Party with ammunition to denounce the prime minister’s leadership during the pandemic.
In “U.K. Is Among First Western Nations to Increase Taxes to Cover COVID-19 Costs,” The Wall Street Journal (WSJ) reported that Labor Party leader Keir Starmer compared Johnson’s tax increases to putting a bandage “on gaping wounds that his party inflicted,” and questioned why they weren’t levied more directly on the rich. The UK government says the wealthiest 14% will pay about half of the extra tax revenues, the WSJ noted.
“This is a tax rise that breaks a promise that the prime minister made at the last election … Read my lips, the Tories can never again claim to be the party of low tax,” Starmer told Reuters.
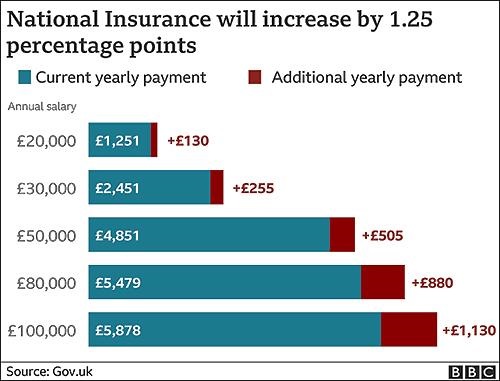
The BBC graphic above illustrates how the tax hikes, which were approved by the Parliament on September 8 by a 319 to 248 vote, will increase the national insurance payroll tax paid by workers and employers by 1.25% each. CNBC reported that the UK government projects the increased taxes will raise £36 billion (US$49.6 billion) over the next three years. (Graphic copyright: BBC.)
Politics versus Hard Facts
According to The Guardian, in 2023-2024, national insurance contributions will be rebranded as a health and social care levy, with more of the money raised going to social care. The added funding will enable the UK government to implement a new cap on total care costs so that no individual will pay more than £86,000 (US$117,142) over their lifetime for social-care programs. Currently, many seniors are forced to sell their homes to meet unexpected care costs, the newspaper noted.
“One message to voters and investors is that taxes are set to rise for years to come,” the WSJ editorial board wrote, predicting the cost of social care will escalate as the UK’s population ages, and that the planned diversion of future taxes for social care will be presented as a “cut” in NHS funding. They maintained that the danger in Johnson’s decision goes deeper than breaking an election campaign pledge or nationalizing more of the UK’s healthcare economy.
“The larger problem is that national healthcare and other entitlements become ever more unaffordable even as they are politically impossible to reform,” the newspaper stated. “The Tories are becoming tax collectors for the entitlement state, which is deadly for parties of the right.”
Bloomberg noted that the UK Institute for Fiscal Studies predicts the planned April 1 tax increase will “raise the UK tax burden to its highest-ever sustained level since records began in 1955—about 35% of national income.”
But, according to the UK-based The Health Foundation, at £2,646.95 (US$3,648.43) per person in 2019, the United Kingdom spends less on healthcare than many developed countries. Less per person than the:
US (£6,782.80),
Germany (£4,131.21),
France (£3,307.54),
Japan (£2,949.19) and
Canada (£2,823.07).
And when healthcare costs are viewed as a percentage of a country’s gross domestic product (GDP), the UK (8% GDP) lags behind the US (13.9%), Germany (9.9%), Japan (9.3%) and France (9.3%) and exceeds only Canada (7.6%) and Italy (6.4%).
While US hospitals, healthcare systems, and patients continue to struggle with ever-increasing healthcare costs, reformers who promote a single-payer healthcare system as an answer to this nation’s healthcare ills may want to take a hard look at the outcomes of the UK’s model.
Clinical laboratory managers and pathologists interested in how the US healthcare system can be improved might be well-served to study the experience of the National Health Service in the UK, that, like all other health systems in the world, has its own unique methods for how it serves its population.
With improved genetic sequencing comes larger human genome databases that could lead to new diagnostic and therapeutic biomarkers for clinical laboratories
As the COVID-19 pandemic grabbed headlines, the human genome database at the US Department of Veterans Affairs Million Veterans Program (MVP) quietly grew. Now, this wealth of genomic information—as well as data from other large-scale genomic and genetic collections—is expected to produce new biomarkers for clinical laboratory diagnostics and testing.
In December, cancer genomics company Personalis, Inc. (NASDAQ:PSNL) of Menlo Park, Calif., achieved a milestone and delivered its 100,000th whole human genome sequence to the MVP, according to a news release, which also states that Personalis is the sole sequencing provider to the MVP.
The VA’s MVP program, which started in 2011, has 850,000 enrolled veterans and is expected to eventually involve two million people. The VA’s aim is to explore the role genes, lifestyle, and military experience play in health and human illness, notes the VA’s MVP website.
Health conditions affecting veterans the MVP is researching include:
The VA has contracted with Personalis through September 2021, and has invested $175 million, Clinical OMICS reported. Personalis has earned approximately $14 million from the VA. That’s about 76% of the company’s revenue, according to 2nd quarter data, Clinical OMICS noted.
“The VA MVP is the largest whole genome sequencing project in the United States, and this is a significant milestone for both the program and for Personalis,” said John West (above with wife Judy), Founder and CEO of Personalis, in the news release. “Population-scale sequencing projects of this nature represent a cornerstone in our effort to accelerate the advancement of precision medicine across a wide range of disease areas,” he added. (Photo copyright: MIT Technology Review.)
Database of Veterans’ Genomes Used in Current Research
What has the VA gained from their investment so far? An MVP fact sheet states researchers are tapping MVP data for these and other veteran health-related studies:
Differentiating between prostate cancer tumors that require treatment and others that are slow-growing and not life-threatening.
How genetics drives obesity, diabetes, and heart disease.
How data in DNA translates into actual physiological changes within the body.
Gene variations and patients’ response to Warfarin.
NIH Research Program Studies Effects of Genetics on Health
Another research program, the National Institutes of Health’s All of Us study, recently began returning results to its participants who provided blood, urine, and/or saliva samples. The NIH aims to aid research into health outcomes influenced by genetics, environment, and lifestyle, explained a news release. The program, launched in 2018, has biological samples from more than 270,000 people with a goal of one million participants.
“We’re changing the paradigm for research. Participants are our most important partners in this effort, and we know many of them are eager to get their genetic results and learn about the science they’re making possible,” said Josh Denny, MD, CEO of the NIH’s All of Us research program in the news release. Denny, a physician scientist, was Professor of Biomedical Informatics and Medicine, Director of the Center for Precision Medicine and Vice President for Personalized Medicine at Vanderbilt University Medical Center prior to joining the NIH. (Photo copyright: National Institutes of Health.)
Inclusive Data Could Aid Precision Medicine
The news release notes that more than 80% of biological samples in the All of Us database come from people in communities that have been under-represented in biomedical research.
“We need programs like All of Us to build diverse datasets so that research findings ultimately benefit everyone,” said Brad Ozenberger, PhD, All of Us Genomics Program Director, in the news release.
Precision medicine designed for specific healthcare populations is a goal of the All of Us program.
“[All of Us is] beneficial to all Americans, but actually beneficial to the African American race because a lot of research and a lot of medicines that we are taking advantage of today, [African Americans] were not part of the research,” Chris Crawford, All of US Research Study Navigator, told the Birmingham Times. “As [the All of Us study] goes forward and we get a big diverse group of people, it will help as far as making medicine and treatment that will be more precise for us,” he added.
Large Databases Could Advance Care
Genome sequencing technology continues to improve. It is faster, less complicated, and cheaper to sequence a whole human genome than ever before. And the resulting sequence is more accurate.
Thus, as human genome sequencing databases grow, researchers are deriving useful scientific insights from the data. This is relevant for clinical laboratories because the new insights from studying bigger databases of genomic information will produce new diagnostic and therapeutic biomarkers that can be the basis for new clinical laboratory tests as well as useful diagnostic assays for anatomic pathologists.
Because of ‘shelter in place’ orders, many anatomic pathologists are reviewing digital images from home during the COVID-19 outbreak and demonstrating the value of whole slide imaging, digital pathology, and CMS’ recent amended remote sign-out policy
COVID-19 is already triggering many permanent changes in the way healthcare is organized and delivered in the United States. However, not until the SARS-CoV-2 pandemic eases will the full extent of these changes become visible. This will be particularly true for anatomic pathology and the profession’s expanded use of telepathology, digital pathology, and whole-slide imaging.
Since early March, specimen referrals and revenues have collapsed at anatomic pathology groups and laboratories across the nation. Dark Daily’s sister publication, The Dark Report (TDR), was first to quantify the magnitude of this collapse in tissue referrals to pathology groups. In an interview with The Dark Report, Kyle Fetter, Executive Vice President and General Manager of Diagnostic Services at XIFIN, Inc., explained that pathology clients using XIFIN’s revenue cycle management services were seeing an average 40% decrease in specimens. And, for certain pathology sub-specialties, the drop-off in specimen referrals was as much as 90%. (See TDR, “From Mid-March, Labs Saw Big Drop in Revenue,” April 20, 2020.)
The College of American Pathologists (CAP) appealed to the Centers for Medicare and Medicaid Services (CMS) to allow pathologists to work remotely. In response, CMS issued a memorandum which stated, “Due to the public health emergency posed by COVID-19 and the urgent need to expand laboratory capacity, CMS is exercising its enforcement discretion to adopt a temporary policy of relaxed enforcement in connection with laboratories located at temporary testing sites under the conditions outlined herein.”
Since then, many physicians, including pathologists, have quickly adapted to working remotely in some form.
Push for Remote Pathology Services Acknowledges Anatomic Pathologist Shortage
The CMS memorandum (QSO-20-21-CLIA), which the federal agency issued to laboratory surveyors on March 26, 2020, notes that CMS will exercise “enforcement discretion to ensure pathologists may review pathology slides remotely” if certain defined conditions are met.
CMS’ decision, which “is applicable only during the COVID-19 public health emergency,” is intended to increase capacity by allowing remote site review of clinical laboratory data, results, and pathology slides.
Ordinarily, CLIA regulations for cytology (a branch of study that focuses on the biological structure of cells) state that cytology slide preparations must be evaluated on the premises of a laboratory that is certified to conduct testing in the subspecialty of cytology. However, a fast-acting Congressional letter sent by 37 members of Congress to US Department of Health and Human Services (HHS) Secretary Alex Azar II, MD, states, “it is unwise and unnecessary to overburden the remaining pathologists with excess work due to staffing shortages, thereby increasing the risk of burnout, medical error, and further shortages in staffing due to exposure. The number of COVID-19 cases will increase and peak over the next two months and will stretch existing healthcare systems to their limits.”
Decreasing Number of ‘Active Pathologists’ Drives Adoption of Telepathology, Digital Pathology, and Whole-slide Imaging
The current COVID-19 outbreak is just the latest factor in support of enabling remote review of anatomic pathology images and cases. The trend of using telepathology, whole-slide imaging (WSI), and digital pathology systems has been gathering momentum for several years. Powerful economic forces support this trend.
The Dark Report devoted its June 10, 2019, issue to a deep dive of the challenges currently facing the anatomic pathology profession. In particular, TDR noted a study published May 31, 2019, in the Journal of the American Medical Association (JAMA) Network Open, titled, “Trends in the US and Canadian Pathologist Workforces from 2007 to 2017.” The study’s authors—pathologists in the United States and Canada—reported that between 2007 and 2017 the number of active pathologists in the United States decreased from 15,568 to 12,839—a 17.53% decline.
TDR noted that these findings imply there are fewer pathologists in the United States today in active practice to handle the steady increase in the number of cases requiring diagnostic review. In turn, this situation could lead to delays in diagnoses detrimental to patient care.
In the United States, the COVID-19 pandemic created an “immediate need for remote sign-outs, reviews, and consults,” said Mike Bonham, MD, PhD (above), Chief Medical Officer for Proscia, a digital pathology software developer, in an interview with Dark Daily. “In the context of highly relevant workflow and workforce challenges, it reinforces the opportunity for wider adoption of digital pathology.” Prior to the outbreak of COVID-19, several distinct forces were driving adoption and use of digital pathology in combination with traditional microscopy, he said. (Photo copyright: Proscia.)
Distinct Forces Beginning to Reshape Anatomic Pathology
In recent years, the anatomic pathology profession has faced growing financial pressure, a shrinking workforce, and a surge in the global demand for pathology—issues that come at a time when biopsies and cancer diagnostics require greater expertise.
The UCSF School of Medicine started with frozen slide sections and moved to the broader volume of pathology slides. Since 2015, UCSF’s School of Medicine has moved toward a fully digital pathology operation and has serialized the adoption by specialty, according to Zoltan Laszik, MD, PhD, attending physician at UCSF and Professor of Clinical Pathology in UCSF’s Departments of Pathology and Laboratory Medicine.
Laszik is among a handful of specialists and digital pathology early adopters who collaborated on the new Dark Daily white paper, which is available for free download.
Through the adoption of digital pathology, glass slides are digitized using a whole-slide image scanner, then analyzed through image viewing software. Although the basic viewing functionality is not drastically different than that provided by a microscope, digitization does bring improvements in lab efficiency, diagnostic accuracy, image management, workflows, and revenue enhancements.
Additionally, artificial intelligence (AI)-based computational applications have emerged as an integral part of the digital pathology workflow in some settings, the white paper explains.
“These developments are important to anatomic pathologists because the traditional pathology business model continues to transform at a steady pace,” noted Robert L. Michel, Editor-in-Chief of The Dark Report.
Anthony Magliocco, MD, FRCPC, FCAP, President and CEO of Protean BioDiagnostics and former Professor and Chair of Pathology at Moffitt Cancer Center, is featured in the white paper as well. His new pathology service model provides routine pathology services, precision oncology, second opinions, liquid biopsies, genetics, and genomics to cancer centers from a Florida-based specialty laboratory.
To register for this important learning opportunity, click here or place this URL in your web browser: https://www.darkdaily.com/webinar/streamlined-operations-increased-revenue-higher-quality-of-care-conclusive-evidence-on-the-value-of-adopting-digital-pathology-in-your-lab/.
These digital pathology technologies represent an innovative movement shaping the present and future of pathology services. Pathologists wanting to learn more are encouraged to sign up for the May 13 webinar, which will build on the body of evidence and commentary that is included in the new white paper, and which will be available for free on-demand download following the live broadcast.
Media reports in the United Kingdom cite bad timing and centralization of public health laboratories as reasons the UK is struggling to meet testing goals
Clinical pathologists and medical laboratories in UK and the US function within radically different healthcare systems. However, both countries faced similar problems deploying widespread diagnostic testing for SARS-CoV-2, the novel coronavirus that causes COVID-19. And the differences between America’s private healthcare system and the UK’s government-run, single-payer system are exacerbating the UK’s difficulties expanding coronavirus testing to its citizens.
The Dark Daily reported in March that a manufacturing snafu had delayed distribution of a CDC-developed diagnostic test to public health laboratories. This meant virtually all testing had to be performed at the CDC, which further slowed testing. Only later that month was the US able to significantly ramp up its testing capacity, according to data from the COVID Tracking Project.
However, the UK has fared even worse, trailing Germany, the US, and other countries, according to reports in Buzzfeed and other media outlets. On March 11, the UK government established a goal of administering 10,000 COVID-19 tests per day by late March, but fell far short of that mark, The Guardian reported. The UK government now aims to increase this to 25,000 tests per day by late April.
This compares with about 70,000 COVID-19 tests per day in
Germany, the Guardian reported, and about 130,000 per day in the US
(between March 26 and April 14), according to the COVID Tracking Project.
“Ministers need to explain why the NHS [National Health Service] is not testing to capacity, why we are falling behind other countries, and what measures they will put in place to address this situation as a matter of urgency,” MP Keir Starmer (above) said in Parliament in late March, The Guardian reported. (Photo copyright: The Guardian.)
What’s Behind the UK’s Lackluster COVID-19 Testing
Response
In January, when the outbreak first hit, Public Health England (PHE) “began a strict program of contact tracing and testing potential cases,” Buzzfeed reported. But due to limited medical laboratory capacity and low supplies of COVID-19 test kits, the government changed course and de-emphasized testing, instead focusing on increased ICU and ventilator capacity. (Scotland, Wales, and Northern Ireland each have separate public health agencies and national health services.)
Later, when the need for more COVID-19 testing became
apparent, UK pathology laboratories had to contend with global shortages of
testing kits and chemicals, The Guardian reported. At present, COVID-19 testing
is limited to healthcare workers and patients displaying symptoms of pneumonia,
acute
respiratory distress syndrome, or influenza-like illness, PHE stated in “COVID-19:
Investigation and Initial Clinical Management of Possible Cases” guidance.
Another factor that has limited widespread COVID-19 testing is the country’s highly-centralized system of public health laboratories, Buzzfeed reported. “This has limited its ability to scale and process results at the same speed as other countries, despite its efforts to ramp up capacity,” Buzzfeed reported. Public Health England, which initially performed COVID-19 testing at one lab, has expanded to 12 labs. NHS laboratories also are testing for the SARS-CoV-2 coronavirus, PHE stated in “COVID-19: How to Arrange Laboratory Testing” guidance.
Sharon Peacock, PhD, PHE’s National Infection Service Interim Director, Professor of Public Health and Microbiology at the University of Cambridge, and honorary consultant microbiologist at the Cambridge clinical and public health laboratory based at Addenbrookes Hospital, defended this approach at a March hearing of the Science and Technology Committee (Commons) in Parliament.
“Laboratories in this country have largely been merged, so we have a smaller number of larger [medical] laboratories,” she said. “The alternative is to have a single large testing site. From my perspective, it is more efficient to have a bigger testing site than dissipating our efforts into a lot of laboratories around the country.”
Writing in The Guardian, Paul Hunter, MB ChB MD, a microbiologist and Professor of Medicine at University of East Anglia, cites historic factors behind the testing issue. The public health labs, he explained, were established in 1946 as part of the National Health Service. At the time, they were part of the country’s defense against bacteriological warfare. They became part of the UK’s Health Protection Agency (now PHE) in 2003. “Many of the laboratories in the old network were shut down, taken over by local hospitals or merged into a smaller number of regional laboratories,” he wrote.
US Facing Different Clinical Laboratory Testing Problems
Meanwhile, a few medical laboratories in the US are now contending with a different problem: Unused testing capacity, Nature reported. For example, the Broad Institute of MIT and Harvard in Cambridge, Mass., can run up to 2,000 tests per day, “but we aren’t doing that many,” Stacey Gabriel, PhD, a human geneticist and Senior Director of the Genomics Platform at the Broad Institute, told Nature. Factors include supply shortages and incompatibility between electronic health record (EHR) systems at hospitals and academic labs, Nature reported.
Politico
cited the CDC’s narrow testing criteria, and a lack of supplies for collecting
and analyzing patient samples—such as swabs and personal protective equipment—as
reasons for the slowdown in testing at some clinical laboratories in the US.
Challenges Deploying Antibody Tests in UK
The UK has also had problems deploying serology tests designed to detect whether people have developed antibodies against the virus. In late March, Peacock told members of Parliament that at-home test kits for COVID-19 would be available to the public through Amazon and retail pharmacy chains, the Independent reported. And, Politico reported that the government had ordered 3.5 million at-home test kits for COVID-19.
However, researchers at the University of Oxford who had been charged with validating the accuracy of the kits, reported on April 5 that the tests had not performed well and did not meet criteria established by the UK Medicines and Healthcare products Regulatory Agency (MHRA). “We see many false negatives (tests where no antibody is detected despite the fact we know it is there), and we also see false positives,” wrote Professor Sir John Bell, GBE, FRS, Professor of Medicine at the university, in a blog post. No test [for COVID-19], he wrote, “has been acclaimed by health authorities as having the necessary characteristics for screening people accurately for protective immunity.”
He added that it would be “at least a month” before suppliers could develop an acceptable COVID-19 test.
In the United States, the Cellex COVID-19 test is intended for use by medical laboratories. As well, many research sites, academic medical centers, clinical laboratories, and in vitro diagnostics (IVD) companies in the US are working to develop and validate serological tests for COVID-19.
Within weeks, it is expected that a growing number of such
tests will qualify for a Food and Drug Administration (FDA) Emergency Use
Authorization (EUA) and become available for use in patient care.