Fear that immunity-resistant mutations of SARS-CoV-2 will emerge are real and the scientific community is paying close attention
Detection of an increasing number of new variants of the SARS-CoV-2 coronavirus raises the possibility that a new strain of COVID-19 might emerge that brings new problems to the management of the pandemic. Public health officials and clinical laboratory scientists are on the alert to determine if any new COVID-19 variant is more virulent or more easily transmissible.
Pathologists, along with the rest of the scientific community worldwide, are following reports of increasing coronavirus mutations with growing concern. The Alpha variant (Lineage B.1.1.7) accounted for most of the COVID-19 cases in April of 2021 in the US, though it was first identified in the United Kingdom. That was followed by the Iota variant (Lineage B.1.526) first identified in New York City. A series of other variants were to follow. Scientists were not surprised. It is normal for viruses to mutate, so they logged and tracked the mutations.
Then, the Delta variant (Lineage B.1.617.2) emerged during a severe outbreak in India. At first, it did not seem more threatening than any other variant, but that changed very quickly. Delta was different.
“The speed with which it dominated the pandemic has left scientists nervous about what the virus will do next. The variant battles of 2021 are part of a longer war, one that is far from over,” The Washington Post reported, which added, “Today, [Delta] has nearly wiped out all of its rivals. The coronavirus pandemic in America has become a Delta pandemic. By the end of July, it accounted for 93.4% of new infections, according to the Centers for Disease Control and Prevention.”
Why is Delta the Worst COVID-19 Variant So Far?
The Delta variant has two advantages that scientists know about:
Stickier spike protein than the spike on the original SARS-CoV-2 coronavirus, as well as on the other, earlier variants. This means that the Delta variant stands a better chance of remaining in a person’s nose or throat long enough to reproduce.
Faster replication. When a virus mutation has more opportunity to reproduce, it quickly becomes the main viral strain. This is the case with the Delta variant. Experts say that the viral load in patients with Delta is around 1,000 times higher than in patients with the original virus.
The image above is a “Colorized scanning electron micrograph of an apoptotic cell (tan) heavily infected with SARS-COV-2 virus particles (orange), isolated from a patient sample,” Newsweek reported. (Photo copyright: National Institute of Allergy and Infectious Diseases/Newsweek.)
Will More Dangerous SARS-CoV-2 Variants Appear?
“The great fear is that nature could spit out some new variant that completely saps the power of vaccines and upends the progress we’ve made against the pandemic. But to virologists and immunologists, such a possibility seems very unlikely,” STAT reported.
That is because, unlike Influenza, which is also a coronavirus, SARS-CoV-2 variants are not able to share genetic materials and recombine into deadlier variants. Thus, scientists are skeptical that a variant could appear and wipe out the progress made with vaccines and treatments.
One of the reasons the Flu vaccine changes every year is Influenza’s ability to recombine into variants that can evade immunity. Therefore, scientists are beginning to suspect that SARS-CoV-2, like the Flu, will likely be around for a while.
“I don’t think eradication is on the table. But I think we could come up with something that’s better than what we have for the flu,” Sharone Green, MD, Associate Professor of Medicine, Division of Infectious Diseases and Immunology and Infection Control Officer at University of Massachusetts Medical School, told Newsweek.
Limiting Infections and Replication
Several factors combined to create the COVID-19 pandemic. But SARS-CoV-2 was a novel coronavirus, meaning it was a new pathogen of a known virus. This meant every person on the planet was a potential host.
The situation now is different. Thanks to natural immunity, vaccines, and treatments that shorten the infection, the SARS-CoV-2 coronavirus has less chance to replicate.
“The pressure is there, but the opportunity is not. The virus has to replicate in order to mutate, but each virus doesn’t get many lottery tickets in a vaccinated person who’s infected,” Jeremy Kamil, PhD, Associate Professor of Microbiology and Immunology at LSU Health in Shreveport, La., told STAT.
Tracking Variants of Interest and Variants of Concern
The World Health Organization (WHO) has been monitoring the viral evolution of SARS-CoV-2 since the beginning of the pandemic. In late 2020, the WHO created categories for tracking variants:
VOIs are “A variant with specific genetic markers that have been associated with changes to receptor binding, reduced neutralization by antibodies generated against previous infection or vaccination, reduced efficacy of treatments, potential diagnostic impact, or predicted increase in transmissibility or disease severity.”
Current VOIs include:
Eta (Lineage B.1.525), detected in multiple countries, designated a VOI in March 2021.
Iota (Lineage B.1.526), US, first detected in November 2020, designated a VOI in March 2021.
Lambda (lineage C.37), Peru, first detected in December 2020, designated a VOI in June 2021.
VOCs, on the other hand, demonstrate all the characteristics of VOIs and also demonstrate “an increase in transmissibility, more severe disease (e.g., increased hospitalizations or deaths), significant reduction in neutralization by antibodies generated during previous infection or vaccination, reduced effectiveness of treatments or vaccines, or diagnostic detection failures.”
Current VOCs include:
Alpha (lineage B.1.1.7), first detected in the UK, September 2020.
Delta (lineage B.1.617.2), first detected in India, October 2020.
Will Vaccines Stop Working?
With each new variant, there tends to be a flurry of media attention and fearmongering. That a variant could emerge which would render our current vaccines ineffective has the scientific community’s attention.
“There is intense interest in whether mutations in the spike glycoprotein mediate escape from host antibodies and could potentially compromise vaccine effectiveness, since spike is the major viral antigen in the current vaccines,” wrote Adam S. Lauring, MD, PhD, and Emma B. Hodcroft, PhD, in “Genetic Variants of SARS-CoV-2—What Do They Mean?” published in the Journal of the American Medical Association (JAMA).
“Because current vaccines provoke an immune response to the entire spike protein, it is hoped that effective protection may still occur despite a few changes at antigenic sites in SARS-CoV-2 variants,” they added.
Future events may justify the optimism that the ongoing effectiveness of vaccines will help with many COVID-19 variants. But pathologists and clinical laboratory leaders may want to be vigilant, because as infection rates increase, so do workloads and demands on critical resources in their medical laboratories.
Report’s authors claim the US needs to be testing 20-million people per day in order to achieve ‘full pandemic resilience’ by August
Medical laboratory scientists and clinical laboratory leaders know that the US’ inability to provide widespread diagnostic testing to detect SARS-CoV-2—the novel coronavirus that causes the COVID-19 illness—in the early stages of the outbreak was a major public health failure. Now a Harvard University report argues the US will need to deliver five million tests per day by early June—more than the total number of people tested nationwide to date—to safely begin reopening the economy.
“We need to deliver five million tests per day by early June to deliver a safe social reopening,” the report’s authors state. “This number will need to increase over time (ideally by late July) to 20 million a day to fully remobilize the economy. We acknowledge that even this number may not be high enough to protect public health. In that considerably less likely eventuality, we will need to scale-up testing much further. By the time we know if we need to do that, we should be in a better position to know how to do it. In any situation, achieving these numbers depends on testing innovation.”
The report is the work of a diverse group of experts in economics, public health, technology, and ethics, from major universities and big technology companies (Apple, Microsoft) with support from The Rockefeller Foundation.
“This is the first plan to show operationally how we can scale up COVID-19 testing sufficiently to safely reopen the economy—while safeguarding fundamental American democratic principles of protecting civil rights and liberties,” Danielle Allen, PhD (above), Director of Harvard University’s Edmond J. Safra Center for Ethics, said in a statement that noted it was “in response to the US Department of Health and Human Service’s Report to Congress on its COVID-19 strategic testing plan.” (Photo copyright: Harvard University.)
Under Harvard’s Roadmap plan, massive-scale testing would involve rapid development of:
Streamlined sample collection (for example) involving saliva samples (spit kits) rather than deep nasal swabs that have to be taken by healthcare workers;
Transportation logistics systems able to rapidly collect and distribute samples for testing;
Mega-testing labs, each able to perform in the range of one million tests per day, with automation, streamlined methods, and tightly managed supply chains;
Information systems to rapidly transmit test results; and
Technology necessary to certify testing status.
“The unique value of this approach is that it will prevent cycles of opening up and shutting down,” Anne-Marie Slaughter, CEO of New America, said in the statement. “It allows us to mobilize and re-open progressively the parts of the economy that have been shut down, protect our frontline workers, and contain the virus to levels where it can be effectively managed and treated until we can find a vaccine.”
Is Expanding Clinical Laboratory Testing Even Possible?
But is such a plan realistic? Perhaps not. When questioned by NBC News about the timeline for “broad-based coronavirus testing” that was suggested as part of the Trump Administration’s three-phase plan to reopen the states, former FDA Commissioner Scott Gottlieb, MD, said, “We’re not going to be there. We’re not going to be there in May, we’re not going to be there in June, hopefully, we’ll be there by September.”
In recent weeks, however, US testing capabilities have improved. Quest Diagnostics, which had come under fire for its testing backlog in California, announced it now has the capacity to perform 50,000 diagnostic COVID-19 tests per day or 350,000 tests per week with less than a two-day turnaround for results. “Our test capacity outpaces demand and we have not experienced a test backlog for about a week,” Quest said in a statement.
CDC ‘Modifies’ Its Guidelines for Declaring a Person ‘Recovered’ from COVID-19
Furthermore, the CDC modified its guidance on the medical and testing criteria that must be met for a person to be considered recovered from COVID-19, which initially required two negative test results before a patient could be declared “confirmed recovered” from the virus. The CDC added a non-testing strategy that allowed states to begin counting “discharged” patients who did not have easy access to additional testing as recovered from the virus.
Under the non-test-based strategy, a person may be considered recovered if:
At least three days (72 hours) have passed since recovery, defined as resolution of fever without the use of fever-reducing medications;
Improvement in respiratory symptoms (e.g., cough, shortness of breath); and,
At least seven days have passed since symptoms first appeared.
For now, however, the focus will likely remain on testing for those who are infected, rather than for finding those who have recovered. As of May 30, the COVID Tracking Project reported that only 16,495,443 million tests had been conducted in the US, with 1,759,693 of those test showing positive for COVID-19. That’s closing in on the 10% “test-positivity rate” recommended by the WHO for controlling a pandemic, but it’s not quite there.
As testing for COVID-19 grows exponentially, clinical laboratories should anticipate playing an increasingly important role in the nation’s response to the COVID-19 pandemic.
Schwan’s concerns about inaccurate or unreliable COVID-19 serology tests were supported when the FDA issued more restrictive rules for these medical laboratory tests on May 4
During a conference call with investors about the company’s first-quarter results, Schwan said of the recently-launched COVID-19 antibody assays, “These tests are not worth anything, or have very little use,” according to reporting from Reuters and other publications. “Some of these companies, I tell you, this is ethically very questionable to get out with this stuff.”
On May 3, Roche announced that its own Elecsys Anti-SARS-CoV-2 antibody test for SARS-CoV-2, the coronavirus that causes the COVID-19 illness, had obtained an emergency use authorization (EUA) from the federal Food and Drug Administration (FDA). In its news release, Roche stated that “the serology test has a specificity greater than 99.8% and sensitivity of 100% (14 days post-PCR confirmation).”
In a separate interview with Bloomberg, Schwan said about antibody testing, “It is very important to pick the right test and then to validate those tests with enough patients.” He then returned to the issue of poor quality in some antibody tests for the SARS-CoV-2 virus, saying, “Unfortunately, there are a number of tests already out there in the market which are not reliable simply because they haven’t been tested sufficiently.”
In reference to the initial release of serological COVID-19 antibody tests, CEO Severin Schwan (above) said during Roche Holding’s first quarter earnings call that, “It’s a disaster. These tests are not worth anything, or have very little use,” reported CNBC. He added, “This is really what matters. Every kind of amateur could produce an antibody test. The two of us could do it overnight in the garage. That’s not the problem. The question is, does it really work? And for that, you have to do testing and validation.” (Photo copyright: Reuters/Arnd Wiegmann.)
A ‘Wild West’ of Unregulated Assays
Prior to issuing tougher rules for how a manufacturer can market a COVID-19 serological test, the FDA had listed about 200 serological tests designed to identify antibodies produced by the human immune system in response to a SARS-CoV-2 infection. This is the process of seroconversion, which is the development of detectable antibodies in a patient’s blood against a pathogen. Detection of IgG antibodies indicates exposure to SARS-CoV-2, according to ARUP Laboratories.
Public health experts have raised questions about the proliferation of such tests for the new coronavirus. Under the FDA’s previous March 16 rules—which were more relaxed than those FDA applied when granting EUAs—the agency was swamped with requests to review more than 200 COVID-19 antibody tests. The looser regulations resulted in nearly no oversight of those tests, reported the Associated Press (AP).
In comments to the AP, Eric Blank, DrPH, Senior Director of Public Health Systems and Programs for the Association for Public Health Laboratories (APHL), said, “Right now it’s a wild west show out there. It really has created a mess that’s going to take a while to clean up.”
“In the meantime,” Blank added, “you’ve got a lot of companies marketing a lot of stuff and nobody has any idea of how good it is.” Blank confirmed to Dark Daily that he made these comments and stands by them.
Calls for Closer Scrutiny of Serological Antibody Tests
In response to the FDA’s March 16 rules for COVID-19 serology tests, APHL requested the federal agency to review its looser approach to reviewing these tests. The impact of the FDA’s much tougher COVID-19 serological testing rules released on May 4 was immediate.
In a press release issued on May 2, the FDA said, “to date, the FDA has authorized 105 tests under EUAs, which include 92 molecular tests, 12 antibody tests, and one antigen test.”
Clinical laboratories in the United States still face difficult challenges if they plan to launch their own COVID-19 serology testing programs. They must select one or more tests from among the antibody and antigen tests that have an FDA EUA. However, data for each of these tests is not as comprehensive as is the data for diagnostic test kits reviewed by the FDA and cleared for market under the pre-market approval process.
This webinar was conducted by James O. Westgard, PhD, and Sten Westgard of Westgard QC, Inc., and the full program is available for free download by clicking here, or by placing this URL in your web browser: https://www.darkdaily.com/webinar/quality-issues-your-clinical-laboratory-should-know-before-you-buy-or-select-covid-19-serology-tests/.
In the webinar recording, the Westgards provide a detailed overview of what elements are required for a clinical lab to have confidence that its COVID-19 serology testing program is producing accurate, reliable results. They explain that labs must understand the unique aspects of the populations they are testing in their communities. All of these factors can then be used by labs to evaluate the different COVID-19 serology tests available for them to purchase, and to select the test that best fits their lab’s capabilities and the characteristics of the patient population that will be tested.
Another important requirement for clinical laboratories to understand is the list of steps necessary to bring up a COVID-19 serological testing program. That starts with validating the test, then bringing it into daily production. As that happens, issues associated with quality control (QC), proficiency testing (PT), and regulatory compliance take center stage, so that the clinical lab has high confidence in the accuracy and reproducibility of the COVID-19 serology test results they are using in patient care or in support of employers who are screening employees for COVID-19.
To register for the June 11 webinar, click here, or place this URL in your web browser: https://www.darkdaily.com/webinar/achieving-high-confidence-levels-in-the-quality-and-accuracy-of-your-clinical-labs-chosen-covid-19-serology-tests/.
New COVID-19 Intelligence from Dark Daily
Announcing Dark Daily’s new COVID-19 STAT Intelligence Briefings! This free service for clinical laboratories, anatomic pathology groups, and diagnostics companies features:
daily breaking news,
business intelligence, and
innovations that clinical labs are using to respond to the COVID-19 pandemic.
This critical information includes effective ways labs can restore their cash flow to pre-pandemic levels and get test claims paid by government and private payers.
One popular feature is the COVID-19 Live! conference calls that happen every Tuesday and Thursday for 30 minutes at 1 PM, EDT. Visit the COVID-19 STAT Intelligence Briefings website and join us for the live calls.
Privacy concerns have one tech giant suggesting alternatives to sharing potentially identifiable location tracking data
Expect an interesting debate on the use of location tracking as a way to manage this and future pandemics. It is a debate that has implications for clinical laboratories. After all, if location tracking identifies individuals who may have been exposed to an infectious disease, will health authorities want those individuals to be immediately tested?
Location tracking has been around for quite some time. Anyone who owns a smartphone knows that digital map and navigation software applications (apps) locate our position and track our movements. That’s how they work. Maps are good. But does collecting and sharing location tracking data violate personal privacy laws that some Silicon Valley tech giants want to use to help public health officials track disease? Maybe.
Google, Facebook, and other tech companies have been talking to the US federal government about ways to use location tracking data from smartphones and online software applications to combat the spread of SARS-CoV-2, the coronavirus that causes the COVID-19 illness, reported the Washington Post.
The tracking data could be used by public health officials
to spot disease outbreaks in populations and predict how it might spread. Analyzing
the data generated by smartphone tracking and reporting apps also could be used
to identify individuals who may have been exposed to the coronavirus, and who should
get clinical laboratory tests to determine if they need medical intervention.
However, Google is apparently resistant to using its collected location data to track and identify individuals. Instead, Google Health’s Head of Communications and Public Affairs, Johnny Luu, said Google was “exploring ways that aggregated anonymized location information could help in the fight against COVID-19. One example could be helping health authorities determine the impact of social distancing, similar to the way we show popular restaurant times and traffic patterns in Google Maps,” said Luu in a statement. He stressed, though, that any such arrangement “would not involve sharing data about any individual’s location, movement, or contacts,” reported the Washington Post.
Can Privacy be Maintained While Tracking Disease?
Google’s sister company, Verily, launched a screening website in March for people who believe they may have COVID-19. The pilot program is only available to some California residents. Users of the service complete a series of online questions to determine their coronavirus risk and whether or not they should seek medical attention.
To use the service, individuals must log into the site using
a Google account and sign a consent authorization form which states data
collected may be shared with public health officials, a move that has received
criticism.
Jacob Snow, JD, a technology and civil liberties attorney with the American Civil Liberties Union (ACLU) of Northern California, expressed concerns about Verily’s program. “COVID-19 testing is a vital public necessity right now—a core imperative for slowing this disease,” he told CNET. “Access to critical testing should not depend on creating an account and sharing information with what is, essentially, an advertising company.
“This is how privacy invasions have the potential to
disproportionately harm the vulnerable,” he continued. “Google should release
this tool without those limits, so testing can proceed as quickly as possible.”
Facebook, on the other hand, has had a Disease Prevention Map program in place for about a year. This program provides location information provided by individuals who choose to participate to health organizations around the globe.
“Disease prevention maps have helped organizations respond to health emergencies for nearly a year and we’ve heard from a number of governments that they’re supportive of this work,” said Laura McGorman, Policy Lead, Data for Good at Facebook, in a statement, reported CNET. “In the coronavirus context, researchers and nonprofits can use the maps, which are built with aggregated and anonymized data that people opt in to share, to understand and help combat the spread of the virus.”
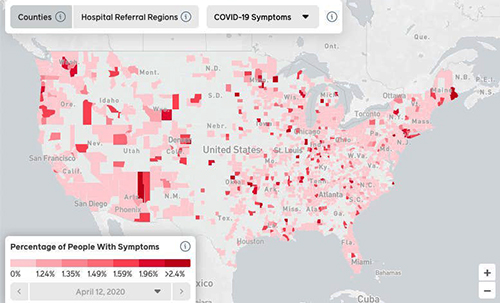
Researchers at Carnegie Mellon University worked with Facebook to create the COVID-19 Symptom Map (above), which is based on aggregated data drawn from self-reported symptoms Facebook. The map, which updates regularly, is viewable by day, counties, hospital referral regions, and COVID-19 symptoms. “This is work that social networks are well-situated to do. By distributing surveys to large numbers of people whose identities we know, we can quickly generate enough signal to correct for biases and ensure sampling is done properly,” wrote Mark Zuckerberg, Facebook founder and CEO, in a Washington Post op-ed about the Carnegie Mellon’s results, reported MobiHealthNews. (Graphic copyright: Facebook/Business Insider.)
Privacy Organizations Voice Concerns
Privacy and civil liberties issues regarding the collection
and use of smartphone data to curtail the pandemic are of concern to some organizations.
There may be legal and ethical implications present when using personal data in
this manner.
Al Gidari, JD, Director of Privacy, Center for Internet and Society at Stanford University Law School, says the balance between privacy and pandemic policy is a delicate one, reported the Washington Post. “The problem here is that this is not a law school exam. Technology can save lives, but if the implementation unreasonably threatens privacy, more lives may be at risk,” he said.
In response to public privacy concerns following the Washington
Post’s report, representatives for Google and Facebook said the companies
have not shared any aggregated and anonymized data with the government
regarding contact
tracing and COVID-19, reported the Washington Post.
Google reiterated that any related projects are still in their early stages and that they are not sure what their participation level might look like. And, CEO Mark Zuckerberg stated that Facebook “isn’t prepared to turn over people’s location data en masse to any governments for tracking the coronavirus outbreak,” reported CNET.
“I don’t think it would make sense to share people’s data in a way where they didn’t have the opportunity to opt in to do that,” Zuckerberg said.
The potential use of location tracking data, when combined
with other information, is one example of how technology can leverage non-medical
information and match it with clinical data to watch population trends.
As of April 23, there were 2,637,911 confirmed cases of COVID-19 and 184,235 deaths from the coronavirus worldwide, according to www.worldometers.info/coronavirus. And, cases of coronavirus disease have been reported in 213 countries according to the World Health Organization (WHO).
As testing increases, more cases will be reported and it is
unknown how long the virus will continue to spread, so advocates of location
tracking and similar technologies that can be brought to bear to save lives during
a disease outbreak may be worth some loss of privacy.
Pathologists and medical laboratory professionals may want
to monitor the public debate over the appropriate use of location tracking.
After all, at some future point, clinical laboratory test results of
individuals might be added to location tracking programs to help public health
authorities better monitor where disease outbreaks are occurring and how they are
spreading.
Media reports in the United Kingdom cite bad timing and centralization of public health laboratories as reasons the UK is struggling to meet testing goals
Clinical pathologists and medical laboratories in UK and the US function within radically different healthcare systems. However, both countries faced similar problems deploying widespread diagnostic testing for SARS-CoV-2, the novel coronavirus that causes COVID-19. And the differences between America’s private healthcare system and the UK’s government-run, single-payer system are exacerbating the UK’s difficulties expanding coronavirus testing to its citizens.
The Dark Daily reported in March that a manufacturing snafu had delayed distribution of a CDC-developed diagnostic test to public health laboratories. This meant virtually all testing had to be performed at the CDC, which further slowed testing. Only later that month was the US able to significantly ramp up its testing capacity, according to data from the COVID Tracking Project.
However, the UK has fared even worse, trailing Germany, the US, and other countries, according to reports in Buzzfeed and other media outlets. On March 11, the UK government established a goal of administering 10,000 COVID-19 tests per day by late March, but fell far short of that mark, The Guardian reported. The UK government now aims to increase this to 25,000 tests per day by late April.
This compares with about 70,000 COVID-19 tests per day in
Germany, the Guardian reported, and about 130,000 per day in the US
(between March 26 and April 14), according to the COVID Tracking Project.
“Ministers need to explain why the NHS [National Health Service] is not testing to capacity, why we are falling behind other countries, and what measures they will put in place to address this situation as a matter of urgency,” MP Keir Starmer (above) said in Parliament in late March, The Guardian reported. (Photo copyright: The Guardian.)
What’s Behind the UK’s Lackluster COVID-19 Testing
Response
In January, when the outbreak first hit, Public Health England (PHE) “began a strict program of contact tracing and testing potential cases,” Buzzfeed reported. But due to limited medical laboratory capacity and low supplies of COVID-19 test kits, the government changed course and de-emphasized testing, instead focusing on increased ICU and ventilator capacity. (Scotland, Wales, and Northern Ireland each have separate public health agencies and national health services.)
Later, when the need for more COVID-19 testing became
apparent, UK pathology laboratories had to contend with global shortages of
testing kits and chemicals, The Guardian reported. At present, COVID-19 testing
is limited to healthcare workers and patients displaying symptoms of pneumonia,
acute
respiratory distress syndrome, or influenza-like illness, PHE stated in “COVID-19:
Investigation and Initial Clinical Management of Possible Cases” guidance.
Another factor that has limited widespread COVID-19 testing is the country’s highly-centralized system of public health laboratories, Buzzfeed reported. “This has limited its ability to scale and process results at the same speed as other countries, despite its efforts to ramp up capacity,” Buzzfeed reported. Public Health England, which initially performed COVID-19 testing at one lab, has expanded to 12 labs. NHS laboratories also are testing for the SARS-CoV-2 coronavirus, PHE stated in “COVID-19: How to Arrange Laboratory Testing” guidance.
Sharon Peacock, PhD, PHE’s National Infection Service Interim Director, Professor of Public Health and Microbiology at the University of Cambridge, and honorary consultant microbiologist at the Cambridge clinical and public health laboratory based at Addenbrookes Hospital, defended this approach at a March hearing of the Science and Technology Committee (Commons) in Parliament.
“Laboratories in this country have largely been merged, so we have a smaller number of larger [medical] laboratories,” she said. “The alternative is to have a single large testing site. From my perspective, it is more efficient to have a bigger testing site than dissipating our efforts into a lot of laboratories around the country.”
Writing in The Guardian, Paul Hunter, MB ChB MD, a microbiologist and Professor of Medicine at University of East Anglia, cites historic factors behind the testing issue. The public health labs, he explained, were established in 1946 as part of the National Health Service. At the time, they were part of the country’s defense against bacteriological warfare. They became part of the UK’s Health Protection Agency (now PHE) in 2003. “Many of the laboratories in the old network were shut down, taken over by local hospitals or merged into a smaller number of regional laboratories,” he wrote.
US Facing Different Clinical Laboratory Testing Problems
Meanwhile, a few medical laboratories in the US are now contending with a different problem: Unused testing capacity, Nature reported. For example, the Broad Institute of MIT and Harvard in Cambridge, Mass., can run up to 2,000 tests per day, “but we aren’t doing that many,” Stacey Gabriel, PhD, a human geneticist and Senior Director of the Genomics Platform at the Broad Institute, told Nature. Factors include supply shortages and incompatibility between electronic health record (EHR) systems at hospitals and academic labs, Nature reported.
Politico
cited the CDC’s narrow testing criteria, and a lack of supplies for collecting
and analyzing patient samples—such as swabs and personal protective equipment—as
reasons for the slowdown in testing at some clinical laboratories in the US.
Challenges Deploying Antibody Tests in UK
The UK has also had problems deploying serology tests designed to detect whether people have developed antibodies against the virus. In late March, Peacock told members of Parliament that at-home test kits for COVID-19 would be available to the public through Amazon and retail pharmacy chains, the Independent reported. And, Politico reported that the government had ordered 3.5 million at-home test kits for COVID-19.
However, researchers at the University of Oxford who had been charged with validating the accuracy of the kits, reported on April 5 that the tests had not performed well and did not meet criteria established by the UK Medicines and Healthcare products Regulatory Agency (MHRA). “We see many false negatives (tests where no antibody is detected despite the fact we know it is there), and we also see false positives,” wrote Professor Sir John Bell, GBE, FRS, Professor of Medicine at the university, in a blog post. No test [for COVID-19], he wrote, “has been acclaimed by health authorities as having the necessary characteristics for screening people accurately for protective immunity.”
He added that it would be “at least a month” before suppliers could develop an acceptable COVID-19 test.
In the United States, the Cellex COVID-19 test is intended for use by medical laboratories. As well, many research sites, academic medical centers, clinical laboratories, and in vitro diagnostics (IVD) companies in the US are working to develop and validate serological tests for COVID-19.
Within weeks, it is expected that a growing number of such
tests will qualify for a Food and Drug Administration (FDA) Emergency Use
Authorization (EUA) and become available for use in patient care.