Researchers used CRISPR-based assays to develop new clinical laboratory point-of-care blood test which boasts accuracy, affordability, and accessibility
According to UPI, the test can “distinguish between influenza A and influenza B—the two main types of seasonal flu—as well as identifying more virulent strains like H1N1 and H3N2.”
Many research teams are working to develop paper-based diagnostic screening tests because of their lower cost to produce and usefulness in remote locations. Should this near-patient point-of-care test become clinically viable, it could mean shorter times to answer, enabling speedier diagnoses and earlier start of treatment.
It also means patient specimens do not have to be transported to a clinical laboratory for testing. And reduced cost per test makes it possible to test more people. This serves the public health aspect of monitoring outbreaks of influenza and other diseases and gives hope for improved treatment outcomes.
“Being able to tease apart what strain or subtype of influenza is infecting a patient has repercussions both for treating them and public health interventions, said Jon Arizti Sanz, PhD, co-lead study author and postdoctoral researcher at the Broad Institute of Harvard and MIT, in a Broad Institute news release.
“Ultimately, we hope these tests will be as simple as rapid antigen tests, and they’ll still have the specificity and performance of a nucleic acid test that would normally be done in a laboratory setting,” Cameron A. Myhrvold, PhD (above), Assistant Professor of Molecular Biology at Princeton University in New Jersey, told CIDRAP. Influenza tests that can be performed at the point of care and in remote locations may reduce the number of screening tests performed by clinical laboratories. (Photo copyright: Michael James Butts/Hertz Foundation.)
Her team developed their tests using Streamlined Highlighting of Infections to Navigate Epidemics (SHINE), “a clustered regularly interspaced short palindromic repeats (CRISPR)-based RNA detection platform,” the researchers wrote in their Journal of Molecular Diagnostics paper.
“SHINE has a runtime of 90 minutes, can be used at room temperature and only requires an inexpensive heat block to heat the reaction. The SHINE technology has previously been used to identify SARS-CoV-2 and later to distinguish between the Delta and Omicron variants,” Bioanalysis Zone reported.
“The test uses genetically engineered enzymes to identify specific sequences of viral RNA in samples,” the researchers told UPI. Originally designed to detect COVID-19, the team adapted the technology to detect influenza in 2022 “with the aim of creating a screening tool that could be used in the field or in clinics rather than hospitals or high-tech diagnostic labs,” they said.
Influenza A and B as well as H1N1 and H3N2 subtypes were the targets of the four SHINE assays. “When tested on clinical samples, these optimized assays achieved 100% concordance with quantitative RT-PCR. Duplex Cas12a/Cas13a SHINE assays were also developed to detect two targets simultaneously,” the researchers wrote in their paper.
The team used “20 nasal swabs from people with flu-like symptoms during the 2020-2021 flu season, nasal fluid from healthy people as the control, and 2016-2021 influenza sequences downloaded from the National Center for Biotechnology Information Influenza (NICB) database. They compared the results with those from quantitative reverse transcription-polymerase chain reaction (RT-PCR) tests,” CIDRAP reported.
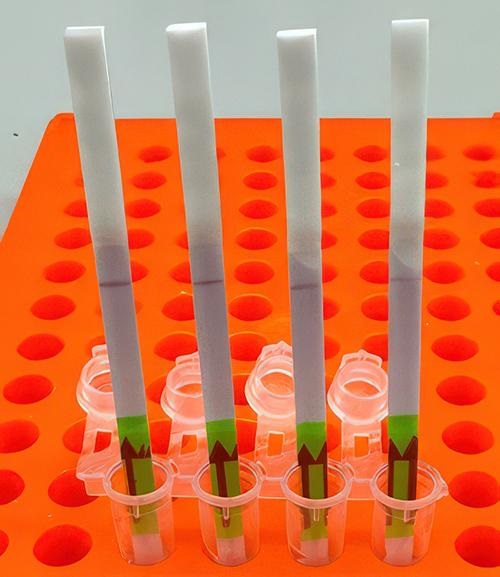
The original 2020 test (shown above) takes 90 minutes to develop at room temperature. The test developers aim to drop this down to 15 minutes. In comparison, typical polymerase chain reaction (PCR) testing requires medical laboratories to have specialized equipment, trained staff, and prolonged processing times, the Broad Institute news release notes. (Photo copyright: Broad Institute.)
Implications of the New Tests
The ease of the new tests is an important development since approximately only 1% of individuals who come down with the flu see doctors for testing, according to the news release. And researchers had this in mind, looking at speed, accuracy, and affordability as a means to “improve outbreak response and infection care around the world,” UPI reported.
There are great benefits to strain differentiation that be achieved with the new test. Doctors are hopeful the test will help dial in the best treatment plans for patients since some strains are resistant to the antiviral medication oseltamivir (Tamiflu), UPI noted. This is significant since Tamiflu “is a common antiviral,” said Sanz in the Broad Institute news release.
“These assays have the potential to expand influenza detection outside of clinical laboratories for enhanced influenza diagnosis and surveillance,” the Journal of Molecular Diagnostics paper noted. This allows for more strategic treatment planning.
“Using a paper strip readout instead of expensive fluorescence machinery is a big advancement, not only in terms of clinical care but also for epidemiological surveillance purposes,” said Ben Zhang, an MD candidate in the Health Sciences and Technology at Harvard and co-first author of the study, in the Broad Institute news release.
Future Plans for Tests
“With further development, the test strip could be reprogrammed to distinguish between SARS-CoV-2 and flu and recognize swine flu and avian flu, including the H5N1 subtype currently causing an outbreak in US dairy cattle,” the study authors told CIDRAP.
The team is also looking at ways to help prevent H5N1 from crossing into human contamination, Sanz told UPI.
The new Princeton/MIT/Harvard tests echo the trend to bring in affordability and ease-of-use with accurate results as an end goal. Faster results mean the best treatments for each person can start sooner and may render the transport of specimens to a clinical laboratory as a second step unnecessary.
As research teams work to develop paper-based viral tests for their plethora of benefits, clinical laboratories will want to pay close attention to this development as it can have a big implication on assisting with future outbreaks.
Additional research is needed before these tests are going to be commonplace in homes worldwide, but this first step brings inspiration and hope of what’s to come.
Clinical laboratory managers and pathology group leaders may want to pay closer attention to shrinking hospital margins and whether this may put pressure on hospital laboratory budgets
Financial performance of the nation’s hospitals and health systems continues to disappoint hospital leaders. For the fourth consecutive month this year, hospital operating margins have remained in the red. This will, of course, affect the clinical laboratories and pathology departments at these institutions.
A recently released National Hospital Flash Report from healthcare management consulting firm Kaufman Hall indicates that 2022 has started off poorly for most healthcare organizations. The information in Kaufman’s report is based on data gathered from more than 900 hospitals and healthcare systems across the country.
The key takeaways outlined in the report for the month of April that are negatively affecting hospitals’ bottom lines include:
More patients are utilizing urgent care facilities, telemedicine options, and primary care providers instead of seeking care at hospital emergency departments.
Patients tend to be sicker, more expensive to treat, and require longer hospital stays compared to April of 2021.
Expenses remain high due to labor shortages, specialty supplies, supply chain issues, and costly pharmaceuticals.
“Labor shortages, high prices for supplies, and cost increases to treat sicker patients over longer stays are ballooning hospital expenses,” Erik Swanson (above), Senior Vice President of Data and Analytics for Kaufman Hall, told Fierce Healthcare. “With a bleak consensus outlook for the US economy, those factors and their effects could be here for a while.” Clinical laboratories have been grappling with supply and personnel shortages and rising costs for many years. (Photo copyright: Kaufman Hall.)
According to the report, the operating margins for the hospitals were down nearly 40% compared to March 2022 and declined 76% when compared to April 2021. The calculated median operating margin index was -3.09% throughout April 2022. In addition, operating earnings declined almost 27% from March to April of this year and 51.5% when contrasted with April of last year.
The report also found that patient volumes, average lengths of stays, and surgeries performed had declined overall during the month of April—but that hospital expenses rose during that period—thus decreasing profit margins. Total expenditures increased by 8.3% over April 2021, and 9.6% between March and April of this year.
Inflation, COVID-19 Key Factors in Hospitals’ First Quarter Losses
The report noted that the historic rise in inflation during the month of April is fueling negative revenues for healthcare systems and hospitals. Several for-profit and nonprofit hospital systems reported losses for the first quarter of 2022.
Kaufman’s report for the month of March was slightly more positive as the healthcare organizations surveyed reported an incremental rise in patient volumes and minor expense relief, resulting in gains in volumes and revenues. March also saw an increase in outpatient and surgery volumes and lower numbers of high-acuity patients. However, that slight upward trend did not last through April.
Another reason for the year-to-date unsatisfactory revenue margins for hospitals across the country was the surge of patients seeking care for the SARS-CoV-2 omicron variant of the COVID-19 infection earlier in the year.
“The first few months of this year were decimated by the impact of the omicron wave, but as the omicron wave subsided, we had a bit of a rebound in those volumes, and that’s what you saw in March,” Erik Swanson, Senior Vice President of Data and Analytics for Kaufman Hall told HealthLeaders. “However, it wasn’t a rebound to the full historical volumes, and that is again because of that wave.”
Healthcare Organizations are Advised to Look at Expenses
The National Hospital Flash Report is published monthly by Kaufman Hall and provides vital analyses and observations on the fiscal performance of hospitals and healthcare systems. The information contained in the report includes data on margins, volumes, revenues, and expenses.
“The revenue side is a bit more challenging for organizations to control. Many are looking at their internal revenue cycle, understanding where there can be improvements in their own process, improving just the performance of the revenue cycle that improves the collections rates,” Swanson said. “Many are also trying to renegotiate with payers and negotiate perhaps as aggressively as possible to get the best rates. But I think where you see much of the levers that organizations can pull is on the expense side.”
Fluctuations in revenue mean that organizations—including clinical laboratories—will have to establish new strategies to diminish their financial shortfalls.
“Finally, because a lot of these challenges are due to these ebbs and flows in volumes, many organizations are also looking to see how they can embrace more data-driven predictive type models to look at volumes and think about how they can optimize their workforce to better handle these ebbs and flows of volume,” Swanson added. “This very often includes thinking about the appropriate size of float pools, the number of times that you need to pay overtime versus hiring new individuals, so many organizations are taking those approaches to bend the cost curve. There are quite a few levers that organizations are pulling to bend this cost curve down to ultimately improve their margins overall.”
The most recent report concluded that the first four months of 2022 have been extremely challenging for hospitals and health systems with extended negative margins taking their toll. The report also projected that the overall picture does not look favorable for these organizations for the remainder of the year and that many healthcare facilities may finish out 2022 with substantially depressed margins.
Clinical laboratory managers and pathology group leaders serving hospital and integrated delivery networks (IDNs) may want to consider how these depressed hospital margins will affect their own laboratories. It may be timely to anticipate how this fall’s budget-planning cycle might require their labs to specify how costs can be cut in the coming budget year.
InspectIR COVID-19 Breathalyzer identifies a chemical signature associated with SARS-CoV-2 in about three minutes with 91.2% sensitivity and 99.3% specificity
One company is hoping that it can make breathalyzers a viable, easier way to screen for SARS-CoV-2. It will soon have the opportunity to learn if consumers will accept this form of screening for COVID-19, as its device recently obtained an Emergency Use Authorization from the FDA.
On April 14, 2022, InspectIR Systems, LLC, of Frisco, Texas, was granted the US Food and Drug Administration’s first-ever emergency use authorization (EUA202006) for a portable breath test device designed to screen for SARS-CoV-2 infection. Clinical laboratories that perform COVID-19 testing will want to compare the high-level sensitivity of this breath test compared to rapid antigen tests currently used for COVID-19 screening.
The device is about the size of a carry-on suitcase. It provides test results in less than three minutes and is currently authorized for use with subjects who are 18 or older.
The FDA’s EUA limits use of the device to “a qualified, trained operator under the supervision of a healthcare provider licensed or authorized by state law to prescribe tests,” the federal agency said. The test “can be performed in environments where the patient specimen is both collected and analyzed, such as doctor’s offices, hospitals, and mobile testing sites.”
The InspectIR COVID-19 Breathalyzer device “is yet another example of the rapid innovation occurring with diagnostic tests for COVID-19,” said Jeffrey Shuren, MD, JD (above), director of the FDA’s Center for Devices and Radiological Health (CDRH), in the news release. A portable device that can identify SARS-CoV-2 infections in a few minutes with 91% specificity may be of great interest to clinical laboratory companies operating COVID-19 popup testing sites around the nation. (Photo copyright: US Food and Drug Administration.)
In granting the authorization, the FDA cited results of a study with 2,409 participants in which the test had sensitivity (correct positive results) of 91.2% and specificity (correct negative results) of 99.3%. “The test performed with similar sensitivity in a follow-up clinical study focused on the Omicron variant,” the agency stated.
“The FDA continues to support the development of novel COVID-19 tests with the goal of advancing technologies that can help address the current pandemic and better position the US for the next public health emergency,” said Jeffrey Shuren, MD, JD, director of the FDA’s Center for Devices and Radiological Health (CDRH), in the news release.
In its coverage of the EUA, CNET noted that the InspectIR breath test is more sensitive than rapid antigen tests but not as sensitive as PCR tests. The FDA advised that people who receive a positive test result with the InspectIR COVID-19 Breathalyzer should follow up with a PCR molecular test.
How the InspectIR COVID-19 Breathalyzer Works
InspectIR LLC was founded in 2017 by Tim Wing and John Redmond, Forbes reported. Their original goal was to develop a breathalyzer for detection of cannabis or opioid use. However, with the onset of the COVID-19 pandemic, the entrepreneurs decided to adapt the technology into a SARS-CoV-2 diagnostic test.
As described in the FDA’s EUA documents, a subject breathes into the device using a sterilized one-time-use straw. A pre-concentrator collects and concentrates the five targeted VOCs, all from the ketone and aldehyde families of organic compounds. These go to a Residual Gas Analyzer, and an algorithm determines whether the sample contains the chemical signature associated with a SARS-CoV-2 infection.
Redmond told Forbes that the specific mix of VOCs is proprietary. The article notes that Wing, Redmond, and Verbeck have patented the pre-concentrator technology.
The devices are manufactured at a Pfeiffer Vacuum Inc. facility in Indiana. The InspectIR founders told Forbes they expect to produce 100 units per week in a start-up phase with plans to ramp up as sales increase. They also plan to look at applications for other respiratory diseases.
InspectIR has not announced exact pricing, but Time reports that the company will lease the equipment to clients, and that pricing per test will be comparable to rapid antigen tests.
InspectIR’s first breathalyzer device is receiving much positive coverage from the media. Should it prove to effective at spotting COVID-19 at popup testing sites, it may supplant traditional clinical laboratory rapid antigen tests as the screening test of choice.
Many of the mutations were found at sites on the spike protein where antibodies bind, which may explain why the Omicron variant is more infectious than previous variants
Scientists at the University of Missouri (UM) now have a better understanding of why the SARS-CoV-2 Omicron variant is more infectious than previous variants and that knowledge may lead to improved antivirals and clinical laboratory tests for COVID-19.
As the Omicron variant of the coronavirus spread across the globe, scientists noted it appeared to be more contagious than previous variants and seemed resistant to the existing vaccines. As time went by it also appeared to increase risk for reinfection.
The UM researchers wanted to know why. They began by examining the Omicron variant’s mutation distribution, its evolutionary relationship to previous COVID-19 variants, and the structural impact of its mutations on antibody binding. They then analyzed protein sequences of Omicron variant samples collected from around the world.
“We know that viruses evolve over time and acquire mutations, so when we first heard of the new Omicron variant, we wanted to identify the mutations specific to this variant,” said Kamlendra Singh, PhD, Associate Research Professor, Department of Veterinary Pathobiology at UM’s College of Veterinary Medicine (CVM), in a UM press release.
Kamlendra Singh, PhD (above), an associate research professor in the Department of Veterinary Pathobiology at UM’s College of Veterinary Medicine, led the team that identified 46 mutations of the SARS-CoV-2 Omicron variant. “I went to India last April and I got infected by the Delta variant. So, it then became personal to me,” he told NBC affiliate KOMU. The UM team hopes their findings lead to improvements in existing COVID-19 antivirals and clinical laboratory tests. (Photo copyright: University of Missouri.)
In their paper, the UM team wrote, “Here we present the analyses of mutation distribution, the evolutionary relationship of Omicron with previous variants, and probable structural impact of mutations on antibody binding. … The structural analyses showed that several mutations are localized to the region of the S protein [coronavirus spike protein] that is the major target of antibodies, suggesting that the mutations in the Omicron variant may affect the binding affinities of antibodies to the S protein.”
There are a total of 46 highly prevalent mutations throughout the Omicron variant.
Twenty-three of the 46 mutations belong to the S protein (more than any previous variant).
Twenty-three of 46 is a markedly higher number of S protein mutations than reported for any SARS-CoV-2 variant.
A significant number of Omicron mutations are at the antibody binding surface of the S protein.
“Mutation is change in the genome that results in a different type of protein,” Singh told NBC affiliate KOMU. “Once you have different kinds of protein after the virus and the virus attacks the cell, our antibodies do not recognize that, because it has already been mutated.”
Omicron Mutations Interfere with Antibody Binding
Of the 46 Omicron variant mutations discovered by the UM researchers, some were found in areas of the coronavirus’ spike protein where antibodies normally bind to prevent infection or reinfection.
“The purpose of antibodies is to recognize the virus and stop the binding, which prevents infection,” Singh explained. “However, we found many of the mutations in the Omicron variant are located right where the antibodies are supposed to bind, so we are showing how the virus continues to evolve in a way that it can potentially escape or evade the existing antibodies, and therefore continue to infect so many people.”
These findings explain how the Omicron variant bypasses pre-existing antibodies in a person’s blood to cause initial infection as well as reinfection.
The UM team hopes their research will help other scientists better understand how the SARS-CoV-2 coronavirus has evolved and lead to future clinical laboratory antiviral treatments.
“The first step toward solving a problem is getting a better understanding of the specific problem in the first place,” Singh said. “It feels good to be contributing to research that is helping out with the pandemic situation, which has obviously been affecting people all over the world.”
Singh and his team have developed a supplement called CoroQuil-Zn designed to reduce a patient’s viral load after being infected with the SARS-CoV-2 coronavirus. The drug is currently being used in parts of India and is awaiting approval from the US Food and Drug Administration (FDA).
New discoveries about SARS-CoV-2 and its variants continue to further understanding of the coronavirus. Research such as that performed at the University of Missouri may lead to new clinical laboratory tests, more effective treatments, and improved vaccines that could save thousands of lives worldwide.
Group’s report also suggests that at-home clinical laboratory tests for COVID-19 that are difficult to use may lead to inaccurate results
At-home clinical laboratory tests for COVID-19 have become quite popular. But how accurate are they? Now, an independent safety organization has investigated COVID-19 rapid antigen tests to find out how easy—or not—they are to use and what that means for the accuracy of the tests’ results.
ECRI (Emergency Care Research Institute) of Plymouth Meeting, Penn., “conducted a usability evaluation to determine if there were any differences in ease of use for the rapid COVID-19 tests,” according to the company’s website.The nonprofit was founded in the 1960s by surgeon and inventor Joel J. Nobel to evaluate medical devices that have been approved by the U.S. Food and Drug Administration (FDA).
“Because of the urgency in providing useful information to consumers as quickly as possible, ECRI selected the seven test kits based on retail availability,” ECRI noted.
ECRI ranked the seven over-the-counter (OTC) at-home rapid antigen tests according to their SUS usability ratings. The System Usability Scale (SUS), invented by John Brooke in 1986, “rates products on a scale of 0 to 100 with 100 being the easiest to use. More than 30 points separated the top and bottom tests analyzed,” according to Managed Healthcare Executive.
Of the seven rapid antigen test kits for COVID-19, ECRI found “noteworthy usability concerns” and “significant differences in ease of use.” None of the tests achieved a SUS rating of “excellent,” ECRI stated in a press release.
“Our evaluation shows that some rapid [COVID-19] tests are much easier to use than others. If given options, consumers should choose tests that are the easiest to use because when a [COVID-19] test is difficult for a consumer to use, it may lead to an inaccurate result,” said ECRI President and CEO Marcus Schabacker, MD, PhD, in a news release. Marcus “is a board-certified anesthesiologist and intensive care specialist with more than 35 years of healthcare experience in complex global environments, and more than 20 years of senior leadership responsibilities serving the medical device and pharmaceutical industries across the healthcare value chain,” states ECRI. (Photo copyright: Biz Journals.)
Seven Rapid Antigen Tests for SARS-CoV-2 Evaluated
As clinical laboratory scientists and pathologists know, it’s possible for different test methodologies for the same biomarker to produce dissimilar results. Another factor affecting medical laboratory test accuracy is the variability from one manufacturing batch or lot to another. And, as the ECRI report suggests, how a specimen is collected and handled can affect accuracy, reliability, and reproducibility of the test results generated by that specimen.
These are the OTC COVID-19 rapid antigen tests ECRI evaluated and their SUS ratings:
Some tests, the ECRI analysts found, required “fine motor control” or were packed with written instructions ECRI determined were too small for older adults to read.
How ECRI Evaluated the COVID-19 Rapid Antigen Tests
SUS reviewers took each rapid test and completed questionnaires specifying their level of agreement (on a range of one to five) with these statements. (Edited by Dark Daily for space):
Desire to use
Perception of unnecessary complexity
Easy to use
Support of a technical person needed
Functions well-integrated
Too much system inconsistency
Easy to learn for most people
A very cumbersome system to use
Feeling of confidence in use
A need to learn before getting going
ECRI then used an algorithm to derive an aggregate score (from 0 to 100) for each test, the report noted.
“Based on the aggregate SUS scores, none of the COVID-19 test kits would be judged to have ‘excellent’ usability. The On/Go, CareStart, Flowflex test kits we rate as ‘very good’ as the usability score for these kits falls just short of ‘excellent,’” the report said.
Some of the positive responses ECRI received from the SUS participants included:
“One of the simpler tests to use with good, printed instructions,” (On/Go and CareStart).
“Cassette makes handling without touching test strip easy,” (CareStart and Flowflex).
“The QR (quick-response) code-linked instructional video is helpful, but probably not needed,” (QuickVue).
“Once the swab is inserted into the test card, the test seems less likely to be spilled or disturbed than other test kits,” (BinaxNOW).
Is it Time for Rapid COVID-19 Antigen Tests?
Unlike RT-PCR tests that can take hours or days to return results, rapid antigen tests provide a quick result that’s used for screening worldwide. And with the COVID-19 Omicron variant spreading rapidly around the world, speed is much needed, according to Stephen Kissler, PhD, Research Fellow in the department of immunology and infectious diseases at Harvard’s T.H. Chan School of Public Health.
“I think the rapid tests provide some of the best protection we have against the spread of disease, especially as we now have a variant on hand that’s going to be able to cause an awful lot of breakthrough infections,” Kissler told The Atlantic-Journal Constitution.
One way clinical laboratory leaders can help is to reach out in their local markets and provide information on the importance of appropriate sampling and collection for accurate results from rapid COVID-19 antigen testing.