By taking early measures to combat the spread, the country had a medical laboratory test for COVID-19 available as early as Jan. 24, and was able to focus medical laboratory testing on the most at-risk individuals
With the Coronavirus disease 2019 (COVID-19) outbreak dominating headlines and medical laboratories under growing pressure to increase testing capacity, Taiwan’s rapid response to the pandemic could provide a critical model for other countries to follow.
Given its proximity to mainland China—just 81 miles—and the large number of individuals who frequently travel back and forth between the countries, Taiwan was at risk of having the second-highest number of imported COVID-19 cases, according to a model developed by researchers at Johns Hopkins University and the University of New South Wales Sydney. News reports indicate that, each year, about 60,000 flights carry 10 million passengers between Taiwan and China.
Data from Taiwan’s Centers for Disease Control (CDC) and Central Epidemic Command Center (CECC) indicate that the country has managed to contain the outbreak thanks to these aggressive actions.
As of March 19, Taiwan’s CECC reported a total of 108 laboratory-confirmed COVID-19 infections. That compares with 81,155 in China, 41,035 in Italy, and 10,755 in the US, according to data compiled by the Center for Systems Science and Engineering at Johns Hopkins University. When the World Health Organization (WHO) reports on the number of COVID-19 cases by country, it includes the number of COVID-19 cases from Taiwan under the totals for the People’s Republic of China. WHO made this decision several years ago, under pressure by China to not recognize Taiwan as an independent nation.
The World
Population Review website says Taiwan’s population is about 23.8 million.
But its infection rate is low even on a per capita basis: Approximately 45
infections per million population, compared with 6,784 in Italy, 564 in China,
and 326 per million in the US.
The JAMA authors noted that Taiwan was prepared for
an outbreak after its experience with the severe
acute respiratory syndrome (SARS) pandemic in 2003, which also originated
in China.
Timeline of COVID-19 Outbreak at the Earliest Stages
Taiwan apparently learned a lesson about preparedness from
the SARS outbreak the rest of the world did not and that enabled the tiny
nation to respond immediately to the novel Coronavirus threat.
The country’s efforts began on Dec. 31 with inspections of
flight arrivals from Wuhan. “When there were only a very few cases [of
COVID-19] reported in China, [Taiwanese health authorities] already went onto
every airplane that came from Wuhan,” C. Jason Wang,
MD, PhD, an Associate Professor of Pediatrics and Director of the Center for Policy, Outcomes, and
Prevention at Stanford University and lead author of the JAMA
report, told Vox.
“Health officials came on the airplane and checked people for symptoms,” he
added.
Travelers who had recently visited Wuhan and displayed
symptoms of pneumonia were quarantined at home for 14 days. Taiwan’s
CDC reported that quarantined individuals were being tested for the
2019-nCoV coronavirus (later renamed to SARS-CoV-2)
soon after it was identified. The CECC, activated in January to coordinate the
government’s response, reported the first confirmed imported case on Jan. 21.
On Jan. 24, their
CDC announced that testing for the virus was being performed at the CDC and
eight designated hospitals. Testing included samples from physicians around the
country. As of Feb. 17, daily testing capacity was about 1,300 samples, the JAMA
authors reported.
Wang told Vox that aggressive measures to identify
and isolate at-risk individuals at the earliest stages reduced the volume of clinical
laboratory tests that had to be performed. “Here in the US and elsewhere, we’re
now seeing community spread,” he said. “It’s probably been here for a while.
And so now we’re trying to see, ‘Oh, how many people should we test?’ Then, you
really need to have a very large capacity in the beginning.”
“I think the US has enormous capacity that’s currently not being used,” C. Jason Wang, MD, PhD (above), Associate Professor of Pediatrics and Director of the Center for Policy, Outcomes, and Prevention at Stanford University and lead author of the JAMA report, told Vox. “We have big tech companies that really could do a lot, right? We ought to get the big companies together. Get the governors together, get the federal government agencies to work with each other, and try to find innovative ways to think about how to best do this. We’ve got the smartest people here in the US because they come from everywhere. But right now, those are untapped resources. They’re not working together. And the federal government, the agencies, they need to collaborate a little more closely.” (Photo copyright: Stanford University.)
More Actions by Authorities
The JAMA report supplementary materials notes a total of 124 actions taken by Taiwanese authorities between Jan. 20 and Feb. 24 to contain the outbreak. In addition to the border inspections, quarantines and testing, they included integration of data between the country’s National Health Insurance Administration and National Immigration Agency, so authorities, and later hospitals, could identify any patient who had recently traveled to China, Hong Kong, or Macau.
The steps also included:
An escalating series of travel restrictions,
eventually including suspension of most passenger flights from Taiwan to China,
as well as a suspension of tours to Hong Kong or Macau.
Use of government-issued cell phones to monitor
quarantined individuals.
Fines for individuals breaking the 14-day home
quarantine.
Fines for incoming travelers who failed to
provide accurate health information.
Fines for disseminating false information or
rumors about the epidemic.
Fines and jail sentences for profiteering on disease-prevention
products.
Designation of military camps and other
government facilities for quarantine.
Nationwide disinfection of universities,
colleges, and public spaces around schools.
The government also took aggressive action to ensure
adequate supplies of surgical masks, including stepped-up manufacturing, export
bans, price limits, and a limit of one to three masks per purchase.
The JAMA authors noted that government officials issued daily press briefings to educate the public about the outbreak. Communication efforts also included public service announcements by Taiwan Vice President Chen Chien-jen, a trained epidemiologist.
A poll taken in Taiwan on Feb. 17 and 18 indicated high approval ratings for officials’ response to the crisis.
The JAMA authors also noted some “challenges” in the
government’s response. For example, most real-time public communication was in
Mandarin Chinese and sign language, leaving out non-Taiwanese citizens in the
country. And the cruise ship Diamond Princess, later found to have infections
on board, was allowed to dock near Taipei and disembark passengers. There are
also questions about whether similar policies can be sustained through the end
of a pandemic.
Still, “well-trained and experienced teams of officials were
quick to recognize the crisis and activated emergency management structures to
address the emerging outbreak,” the JAMA authors wrote. “Taiwan is an
example of how a society can respond quickly to a crisis and protect the
interests of its citizens.”
One noteworthy difference in the speedy response to
recognition of a novel coronavirus in Taiwan, compared to recognition of the
same novel coronavirus in the United States, was the fast availability of
clinical laboratory tests for COVID-19 in Taiwan.
Pathologists and clinical laboratory professionals here in
the US are frustrated that their skills and talents at developing and
validating new assays on an accelerated timeline were not acknowledged and
leveraged by government officials as they decided how to respond to the
emergence of the novel coronavirus now called SARS-CoV-2.
In a separate study, HHS finds a 40% increase in sepsis cases, as more patients succumb to infections without effective antibiotics and antimicrobial drugs
Given the drastic steps being taken to slow the spread of the Coronavirus in America, it’s easy to forget that significant numbers of patients die each year due to antibiotic-resistant bacteria (ARB), other forms of antimicrobial resistance (AMR), and in thousands of cases the sepsis that follows the infections.
The CDC’s website states that “more than 2.8 million antibiotic-resistant infections occur in the US each year, and more than 35,000 people die as a result.” And a CDC news release states, “on average, someone in the United States gets an antibiotic-resistant infection every 11 seconds and every 15 minutes someone dies.”
Those are huge numbers.
Clinical laboratory leaders and microbiologists have learned to be vigilant as it relates to dangerously infectious antimicrobial-resistant agents that can result in severe patient harm and death. Therefore, new threats identified in the CDC’s Antibiotic Resistance Threats in the United States report will be of interest.
Drug-resistant Microbes That Pose Severe Risk
The CDC has added the fungus Candida auris (C. auris) and carbapenem-resistant Acinetobacter (a bacteria that can survive for a long time on surfaces) to its list of “urgent threats” to public health, CDC said in the news release. These drug-resistant microbes are among 18 bacteria and fungi posing a greater threat to patients’ health than CDC previously estimated, Live Science reported.
In 2013, the CDC estimated that about two million people each year acquired an antibiotic-resistant (AR) infection that killed as many as 23,000. However, in 2019, the CDC reported that those numbers were low and that the number of deaths due to AR infections in 2013 was about twice that amount. During a news conference following the CDC announcement, Michael Craig (above), a Senior Adviser for the CDC’s Antibiotic Resistance Coordination and Strategy Unit said, “We knew and said [in 2013] that our estimate was conservative … and we were right,” Live Science reported. In 2019, CDC reported 2.8 million antibiotic-resistant infections annually with more than 35,000 related deaths in the US alone. (Photo copyright: Centers for Disease Control and Prevention.)
The CDC considers five threats to be urgent. Including the
latest additions, they are:
Dark Daily has regularly covered the healthcare industry’s ongoing struggle with deadly fungus and bacteria that are responsible for hospital-acquired infections (HAI) and sepsis. This latest CDC report suggests healthcare providers continue to struggle with antimicrobial-resistant agents.
Acinetobacter Threat Increases and C. auris
a New Threat since 2013
Carbapenem-resistant Acinetobacter, a bacterium that
causes pneumonia and bloodstream and urinary tract infections, escalated from
serious to urgent in 2013. About 8,500 infections and 700 deaths were noted by the
CDC in 2017.
C. auris, however, was not addressed in the 2013
report at all. “It’s a pathogen that we didn’t even know about when we wrote
our last report in 2013, and since then it’s circumvented the globe,” said Michael
Craig, Senior Adviser for the CDC’s Antibiotic Resistance Coordination and
Strategy Unit, during a news conference following the CDC announcement, Live
Science reported.
Today, C. auris is better understood. The fungus
resists emerging drugs, can result in severe infections, and can be transmitted
between patients, CDC noted.
By year-end, CDC tracking showed 988 cases in the US.
More Patients Getting Sepsis as Antibiotics Fail: HHS
Study
In a separate study published in Critical Care Medicine, a journal of the Society of Critical Care Medicine (SCCM), the US Department of Health and Human Services (HHS) found that antibiotic-resistant bacteria and fungi are resulting in more people acquiring sepsis, a life-threatening condition, according to an HHS news release.
Sepsis increased by 40% among hospitalized Medicare patients
from 2012 through 2018, HHS reported.
“These (untreatable infections) are happening here and now in the United States in large numbers. This is isn’t some developing world thing. This isn’t a threat for 2050. It’s a threat for here and now,” Cornelius “Neil” Clancy, MD, Associate Chief of Veterans Affairs Pittsburg Health System (VAPHS) and Opportunistic Pathogens, told STAT.
It is troubling to see data about so many patient deaths
related to antibiotic-resistant infections and sepsis cases when the world is
transfixed by the Coronavirus. Nevertheless, it’s important that medical laboratory
leaders and microbiologists keep track of how the US healthcare system is or is
not responding to these new infectious agents. And, to contact infection
control and environmental services colleagues to enhance surveillance, ensure
safe healthcare environments and equipment, and adopt appropriate strategies to
prevent antibiotic-resistant infections.
Researchers are discovering it’s possible to determine a person’s age based on the amount of protein in the blood, but the technology isn’t always correct
Mass spectrometry is increasingly finding its way into clinical laboratories and with it—proteomics—the study of proteins in the human body. And like the human genome, scientists are discovering that protein plays an integral part in the aging process.
This is a most interesting research finding. Might medical laboratories someday use proteomic biomarkers to help physicians gauge the aging progression in patients? Might this diagnostic capability give pathologists and laboratory leaders a new product line for direct-to-consumer testing that would be a cash-paying, fast-growing, profitable clinical laboratory testing service? If so, proteomics could be a boon to clinical laboratories worldwide.
When research into genomics was brand-new, virtually no one imagined that someday the direct-to-consumer lab testing model would offer genetic testing to the public and create a huge stream of revenue for clinical laboratories that process genetic tests. Now, research into protein and aging might point to a similar possibility for proteomics.
For example, through proteomics, researchers led by Benoit Lehallier, PhD, Biostatistician, Instructor of Neurology and Neurological Sciences, and senior author Tony Wyss-Coray, PhD, Professor of Neurology and Neurological Sciences and co-director of the Stanford Alzheimer’s Disease Research Center at Stanford University in California, gained an understanding of aging that suggest intriguing possibilities for clinical laboratories.
In their study, published in Nature, titled, “Undulating Changes in Human Plasma Proteome Profiles Across the Lifespan,” the scientists stated that aging doesn’t happen in a consistent process over time, reported Science Alert.
The Stanford researchers also found that they can accurately
determine a person’s age based on the levels of certain proteins in his or her
blood.
Additionally, the study of proteomics may finally explain why blood from young people can have a rejuvenating effect on elderly people’s brains, noted Scientific American.
Each of these findings is important on its own, but taken
together, they may have interesting implications for pathologists who follow
the research. And medical laboratory leaders may find opportunities in mass
spectrometry in the near future, rather than decades from now.
Three Distinct Stages in Aging and Other Findings
The Stanford study found that aging appears to happen at
three distinct points in a person’s life—around the ages 34, 60, and 78—rather
than being a slow, steady process.
The researchers measured and compared levels of nearly 3,000
specific proteins in blood plasma taken from healthy people between the ages of
18 and 95 years. In the published study, the authors wrote, “This new approach
to the study of aging led to the identification of unexpected signatures and
pathways that might offer potential targets for age-related diseases.”
Along with the findings regarding the timeline for aging, the researchers found that about two-thirds of the proteins that change with age differ significantly between men and women. “This supports the idea that men and women age differently and highlights the need to include both sexes in clinical studies for a wide range of diseases,” noted a National Institutes of Health (NIH) report.
“We’ve known for a long time that measuring certain proteins in the blood can give you information about a person’s health status—lipoproteins for cardiovascular health, for example,” stated Wyss-Coray in the NIH report. “But it hasn’t been appreciated that so many different proteins’ levels—roughly a third of all the ones we looked at—change markedly with advancing age.”
Tony Wyss-Coray, PhD (above), Professor of Neurology and Neurological Sciences at Stanford University, was senior author of the proteomics study that analyzed blood plasma from 4,263 people between the ages 18-95. “Proteins are the workhorses of the body’s constituent cells, and when their relative levels undergo substantial changes, it means you’ve changed, too,” he said in a Stanford Medicine news article. “Looking at thousands of them in plasma gives you a snapshot of what’s going on throughout the body.” (Photo copyright: Stanford University.)
Differentiating Aging from Disease
Previous research studies also found it is indeed possible
to measure a person’s age from his or her “proteomic signature.”
The researchers published their findings in Aging Cell, a peer-reviewed open-access journal of the Anatomical Society in the UK, titled, “Plasma Proteomic Signature of Age in Healthy Humans.” In it, the authors wrote, “Our results suggest that there are stereotypical biological changes that occur with aging that are reflected by circulating proteins.”
The fact that chronological age can be determined through a
person’s proteomic signature suggests researchers could separate aging from
various diseases. “Older age is the main risk factor for a myriad of chronic
diseases, and it is invariably associated with progressive loss of function in
multiple physiological systems,” wrote the researchers, adding, “A challenge in
the field is the need to differentiate between aging and diseases.”
Can Proteins Cause Aging?
Additionally, the Stanford study found that changes in protein levels might not simply be a characteristic of aging, but may actually cause it, a Stanford Medicine news article notes.
“Changes in the levels of numerous proteins that migrate
from the body’s tissues into circulating blood not only characterize, but quite
possibly cause, the phenomenon of aging,” Wyss-Coray said.
Can Proteins Accurately Predict Age? Not Always
There were, however, some instances where the protein levels inaccurately predicted a person’s age. Some of the samples the Stanford researchers used were from the LonGenity research study conducted by the Albert Einstein College of Medicine, which investigated “why some people enjoy extremely long life spans, with physical health and brain function far better than expected in the 9th and 10th decades of life,” the study’s website notes.
That study included a group of exceptionally long-lived Ashkenazi Jews, who have a “genetic proclivity toward exceptionally good health in what for most of us is advanced old age,” according to the Stanford Medicine news article.
“We had data on hand-grip strength and cognitive function
for that group of people. Those with stronger hand grips and better measured
cognition were estimated by our plasma-protein clock to be younger than they
actually were,” said Wyss-Coray. So, physical condition is a factor in
proteomics’ ability to accurately prediction age.
Although understanding the connections between protein in
the blood, aging, and disease is in early stages, it is clear additional
research is warranted. Not too long ago the idea of consumers having their DNA
sequenced from a home kit for fun seemed like fantasy.
However, after multiple FDA approvals, and the success of
companies like Ancestry, 23andMe, and the clinical laboratories that serve them,
the possibility that proteomics might go the same route does not seem so
far-fetched.
At The Dark Report’s annual Lab Quality Confab for clinical laboratory administrators, managers, and quality team members, experts outline how disruption in healthcare requires labs to improve processes and cut costs
This is an opportunity for clinical laboratory directors,
pathologists, and other lab professionals, to comment on the proposed revisions
to CLIA before or during the upcoming CLIAC meeting on Nov. 6.
The agenda for the meeting is posted on the CDC’s website.
Public to be Heard on CLIA Regulations
“For the first time in its 26-year history, the council has
called for three workgroups to address how to revise CLIA,” Salerno said. The
workgroups will address these topics:
“It’s a dramatic step for the government to ask the
laboratory community how to revise the CLIA regulations,” Salerno commented.
Chartered in 1992, the advisory council meets twice a year, once in April and
once in November.
In the coming weeks, Dark Daily will publish more
information on how clinical laboratory professionals can comment on the
important issue of CLIA revisions.
Digital slides from Salerno’s keynote address are posted on LQC’s presentations website.
Clinical Laboratory Testing is Increasing in Value,
Keynote Speaker Says
As a service to clinical laboratories, Salerno outlined many
of the services the CDC’s Division of Laboratory Systems provides for free to
clinical labs, including information on such topics as:
During his remarks at the 13th Annual Lab Quality Confab in Atlanta, Salerno had good news for the clinical laboratory professionals in attendance. He said that lab testing was becoming a more valued commodity in healthcare because physicians and other providers were growing increasingly confident in lab test results. [Photo copyright: The Dark Report.]
Healthcare System Disruption Impacts Providers, Including
Clinical Laboratories
Other keynote speakers addressed how disruption in the US
healthcare systems affects provider organizations in significant ways. For
clinical laboratories, such disruption has resulted in reduced payment and
demands for quality improvement and shorter turnaround times.
For all these reasons, quality
management systems may be every clinical laboratory’s best strategy to
survive and thrive, the keynote speakers said.
The first keynoter was Robert L. Michel, Editor-in-Chief and Publisher of The Dark Report. Michel’s remarks focused on how price cuts from Medicare, Medicaid, private payers, and the drive for value-based payment, are requiring labs to do more with less. For this reason, quality management systems are necessary for all labs seeking to improve results, eliminate errors, and cut costs, he said.
“The people closest to the work know how to fix these
problems,” he added. “That’s why labs know they must train their staff to
identify problems and then report them up the chain so they can be fixed,”
Michel commented. “Labs that are best at listening to their employees are
getting very good at identifying problems by measuring results and monitoring
and reporting on their own performance.”
Michel identified three principle factors that are
disrupting healthcare:
The shift from reactive care in which the health system cares for sick patients to proactive care in which the health system aims to keep patients healthy and out of the hospital and other costly sites of care.
The transition away from fee-for-service payment that encourages providers to do more for patients, whether more care is needed or not, to value-based payment that aims to reward providers for keeping patients healthy.
The consolidation among hospitals, health systems, physicians, and other providers. A trend that requires clinical laboratories to find new partners and new ways to improve lab services and reduce costs.
Informatics Performance Data Help Clinical Laboratories
Respond to Change
“The attributes of new and successful labs are that they will have faster workflow and shorter cycle times for clinical lab tests and anatomic pathology specimen results,” Michel explained. “That means that labs will attack non-value-added processes by implementing continuous improvement strategies [such as Lean and Six Sigma] and by the sophisticated use of informatics.”
Making use of performance data enables clinical laboratory
directors to make changes in response to disruptions that affect healthcare.
“If you have good informatics, then seven or eight of every 10 decisions you
make will be good decisions, and with the other two and three decisions, you’ll
have time to pull back and adjust,” Michel commented.
The second keynote speaker, Jeremy Schubert, MBA, MPH, Division Vice President of Abbott, reiterated what Michel said about how the health system is moving away from fee-for-service payment. Instead of focusing on caring for sick patients exclusively, he said, health insurers are paying all healthcare providers to keep patients healthy.
“Healthcare today is about the whole life course of the
individual,” Schubert explained. “Patients no longer want healthcare only when
they’re sick. Instead, they want to be healthy. And health creation is not just
about a person’s physical health. It’s about their mental health, their
emotional health, and their social wellbeing.
“In fact,” he continued, “you can learn more about a
person’s health from their Zip code than from their genetic code.”
That is essentially what TriCore Reference Laboratories (TriCore) has been doing in New Mexico, Schubert added. During his presentation, Michel mentioned TriCore as being one of four clinical laboratories participating in Project Santa Fe, a non-profit organization that promotes the movement from Clinical Lab 1.0 to Clinical Lab 2.0. (See “TriCore Forges Ahead to Help Payers Manage Population Health,” The Dark Report, May 20, 2019.)
“If you want to be a quality engine in healthcare you have
to be operating at Lab 2.0. Who is best qualified to interpret information?
It’s the lab,” Schubert said. Then he challenged labs to begin pursuing the
goal of achieving Lab 3.0, saying “Lab 3.0 is being able to interface with the
patient to address each patient’s problems.”
The 13th Annual Lab Quality Confab (LQC) in Atlanta continues through the 17th with post-event workshops in Six Sigma and mastering quality management systems. In attendance are 300 clinical laboratory administrators, managers, and quality team members who are learning a complete array of professional training methods.
To register to attend, click here or enter https://www.labqualityconfab.com/register into your browser, or call 707-829-9485, or e-mail lqcreg@amcnetwork.com.
US hospitals typically spend $2,424/day to provide inpatient care, according to the KFF report
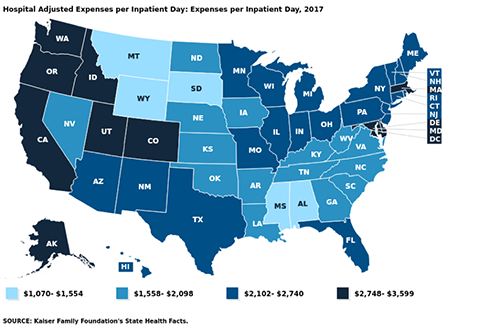
How much does the average hospital spend/day to provide inpatient care? The numbers vary widely, but the latest statistics from Kaiser Family Foundation (KFF) State Health Facts show West Coast states incur the highest daily operating and non-operating inpatient costs.
This disparity in spending is unlikely to surprise medical laboratory executives working in hospital settings. They know firsthand that operating costs can vary from state-to-state and by hospital ownership type.
Oregon, California, and Washington are the most expensive
three states overall for inpatient hospital care. However, the leaderboard
changes when looking specifically at inpatient care at for-profit hospitals.
In the for-profit hospital category:
North Dakota, South Dakota, and Alaska rack up
the highest expenses/day.
Idaho, California, and Oregon top the non-profit
hospital segment.
Overall in the US, the average hospital incurs expenses of
$2,424/inpatient day, the KFF reports.
While the average US hospital spends $2,424/day to deliver inpatient care, West Coast states have the highest hospital adjusted operating and non-operating expenses/inpatient day, according to a recent report from the Kaiser Family Foundation. Oregon hospitals top the spending list at $3,599/day. (Graphic copyright: Kaiser Family Foundation.)
AMA Annual Survey
Rankings
Rankings are based on information from the 1999-2017 American Hospital
Association Annual Survey, which includes all operating and non-operating
expenses for registered US community hospitals. The figures are an estimate of
the expenses incurred by a hospital to provide a day of inpatient care. They
have been adjusted higher to reflect an estimate of the volume of outpatient
services, according to the KFF. The numbers do not reflect actual charges or
reimbursement for the care provided.
Most expensive average expenses/inpatient day:
Oregon, $3,599
California, $3,441
Washington, $3,429
Idaho, $3,119
District of Columbia, $3,053
Least expensive average expenses/inpatient day:
Montana, $1,070
Mississippi, $1,349
South Dakota, $1,505
Wyoming, $1,520
Alabama, $1,554
Most expensive non-profit hospitals/inpatient day:
Idaho, $4,208
California, $3,800
Oregon, $3,546
Washington, $3,500
Colorado, $3,319
Least expensive non-profit hospitals/inpatient day:
Mississippi, $1,365
South Dakota, $1,519
Iowa, $1,564
Montana, $1,627
Alabama, $1,723
Most expensive for-profit hospitals/inpatient day:
North Dakota, $4,701
South Dakota, $3,956
Alaska, $3,280
Nebraska, $3,031
Wisconsin, $2,830
Least expensive for-profit hospitals/inpatient day:
Maine, $1,055
Maryland, $1,207
West Virginia, $1,362
Iowa, $1,558
Arkansas, $1,619
Most expensive state/local government hospitals/inpatient
day:
Oregon, $4,062
Connecticut, $3,979
Washington, $3,312
California, $3,217
Utah, $3,038
Least expensive state/local government hospitals/inpatient
day:
Montana, $52
South Dakota, $442
Pennsylvania, $787
Nebraska, $906
Georgia, $917
Some Regions Pay Much
More for Healthcare
The KFF report did not look at whether patients in states
where hospitals incur the highest daily operating and non-operating expenses
also pay the most for hospital services. Hospital charges vary widely, with
many treatments costing far more in some regions than others.
In addition, health bills can vary at different hospitals in
the same city or region. According to Healthcare.gov,
the average total cost of a three-day hospital stay is about $30,000.
Adding to the confusion is the fact that hospital costs,
billed charges, and the amounts paid by patients for services can be distinctly
different amounts. Health insurance companies, for example, negotiate lower
rates with hospitals and health systems for their plan enrollees. While patients
without insurance are billed full price for services based on the hospital’s chargemaster.
Zack Cooper, PhD, Associate Professor of Health Policy and Economics at Yale University, told National Public Radio (NPR) that hospital consolidation is partly to blame for the wide variation in the price of hospital services within states and across the country. He says consolidation has eliminated competition in many markets. “Where one large hospital dominates the markets, that hospital is able to get higher prices,” Cooper maintains. “Hospitals have gotten increasingly powerful over time.” (Photo copyright: Yale University.)
CMS Final Rule
Requires Pricing Transparency
As of Jan. 1, 2019, a new Centers for Medicare and Medicaid Services (CMS) rule went into effect aimed at making hospital pricing more transparent. The CMS is now requiring hospitals to publish chargemaster price lists online, rather than release those numbers to patients upon request.
However, healthcare advocates have questioned the rule’s
impact on transparency. Posted hospital pricing information is often hard to
access and difficult to comprehend. In addition, chargemaster prices typically
do not represent the actual costs passed on to consumers.
“[The chargemaster] is the list price. When you go to buy a car, you have a manufacturer’s suggested retail price. This is basically what [the chargemaster] is,” Medical Contributor Natalie Azar, MD, told NBC News.
“Prevention comes first,” Nechrebecki suggests. “Utilize the
ambulatory care clinics. Go see your doctors and do what they recommend to keep
yourself healthy. Eat well and exercise often. You will prevent many surgeries
and hospitalizations.”
Sound advice. Nevertheless, clinical laboratories and anatomic pathology groups should take note of the federal government’s ongoing push for price transparency and prepare accordingly.