Medical laboratories are already using gene sequencing as part of a global effort to identify new variants of the coronavirus and their genetic ancestors
Thanks to advances in genetic sequencing technology that enable medical laboratories to sequence organisms faster, more accurately, and at lower cost than ever before, clinical pathology laboratories worldwide are using that capability to analyze the SARS-CoV-2 coronavirus and identify variants as they emerge in different parts of the world.
The US Centers for Disease Control and Prevention (CDC) now plans to harness the power of gene sequencing through a new consortium called SPHERES (SARS-CoV-2 Sequencing for Public Health Emergency Response, Epidemiology, and Surveillance) to “coordinate SARS-CoV-2 sequencing across the United States,” states a CDC news release. The consortium is led by the CDC’s Advanced Molecular Detection (AMD) program and “aims to generate information about the virus that will strengthen COVID-19 mitigation strategies.”
The consortium is comprised of 11 federal agencies, 20 academic institutions, state public health laboratories in 21 states, nine non-profit research organizations, and 14 lab and IVD companies, including:
Abbott Diagnostics
bioMérieux
Color Genomics
Ginkgo Bioworks
IDbyDNA
Illumina
In-Q-Tel
LabCorp
One Codex
Oxford Nanopore Technologies
Pacific Biosciences
Qiagen
Quest Diagnostics
Verily Life Sciences
‘Fundamentally Changing How Public Health Responds’
Gene sequencing and related technologies have “fundamentally changed how public health responds in terms of surveillance and outbreak response,” said Duncan MacCannell, PhD, Chief Science Officer for the CDC’s Office of Advanced Molecular Detection (OAMD), in an April 30 New York Times (NYT) article, which stated that the CDC SPHERES program “will help trace patterns of transmission, investigate outbreaks, and map how the virus is evolving, which can affect a cure.”
The CDC says that rapid DNA sequencing of SARS-CoV-2 will help monitor significant changes in the virus, support contact tracing efforts, provide information for developers of diagnostics and therapies, and “advance public health research in the areas of transmission dynamics, host response, and evolution of the virus.”
The sequencing laboratories in the consortium have agreed to “release their information into the public domain quickly and in a standard way,” the NYT reported, adding that the project includes standards for what types of information medical laboratories should submit, including, “where and when a sample was taken,” and other critical details.
Even in its early phase, the CDC’s SPHERES project has “made a tangible impact in the number of sequences we’re able to deposit and make publicly available on a daily basis,” said Pavitra Roychoudhury, PhD (above), Acting Instructor and Senior Fellow at the University of Washington, and Research Associate at Fred Hutchinson Cancer Research Center, in an e-mail to the NYT. “What we’re essentially doing is reading these small fragments of viral material and trying to jigsaw puzzle the genome together,” said Roychoudhury in an April 28 New York Times article which covered in detail how experts are tracking the coronavirus since it arrived in the US. (Photo copyright: LinkedIn.)
Sharing Data Between Sequencing Laboratories and Biotech Companies
The CDC announced the SPHERES initiative on April 30, although it launched in early April, the NYT reported.
According to the CDC, SPHERES’ objectives include:
To bring together a network of sequencing laboratories, bioinformatics capacity and subject matter expertise under the umbrella of a massive and coordinated public health sequencing effort.
To identify and prioritize capabilities and resource needs across the network and to align sources of federal, non-governmental, and private sector funding and support with areas of greatest impact and need.
To improve coordination of genomic sequencing between institutions and jurisdictions and to enable more resilience across the network.
To champion concepts of openness, standards-based analysis, and rapid data sharing throughout the United States and worldwide during the COVID-19 pandemic response.
To provide a common forum for US public, private, and academic institutions to share protocols, methods, bioinformatics tools, standards, and best practices.
To establish consistent data and metadata standards, including streamlined repository submission processes, sample prioritization criteria, and a framework for shared, privacy-compliant unique case identifiers.
To align with other national sequencing and bioinformatics networks, and to support global efforts to advance the use of standards and open data in public health.
Implications for Developing a Vaccine
As the virus continues to mutate and evolve, one question is whether a vaccine developed for one variant will work on others. However, several experts told The Washington Post that the SARS-CoV-2 coronavirus is relatively stable compared to viruses that cause seasonal flu (influenza).
“At this point, the mutation rate of the virus would suggest that the vaccine developed for SARS-CoV-2 would be a single vaccine, rather than a new vaccine every year like the flu vaccine,” Peter Thielen, a molecular biologist at the Johns Hopkins University Applied Physics Laboratory, told the Washington Post.
Nor, he said, is one variant likely to cause worse clinical outcomes than others. “So far, we don’t have any evidence linking a specific virus [strain] to any disease severity score. Right now, disease severity is much more likely to be driven by other factors.”
Fast improvements in gene sequencing technology have made it faster, more accurate, and cheaper to sequence. Thus, as the COVID-19 outbreak happened, there were many clinical laboratories around the world with the equipment, the staff, and the expertise to sequence the novel coronavirus and watch it mutate from generation to generation and from region to region around the globe. This capability has never been available in outbreaks prior to the current SARS-CoV-2 outbreak.
Limited availability of COVID-19 clinical lab tests is major topic at federal briefings and news stories, yet many of nation’s labs are laying off staff and at point of closing
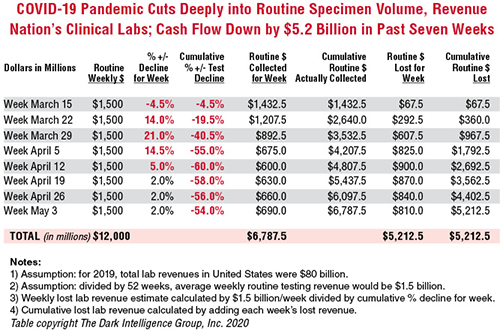
Cash flow at the nation’s clinical laboratories has crashed, with revenues down by more than $5 billion since early March. This is the biggest financial disaster for the nation’s clinical laboratory industry in its 100-year history and it couldn’t come at a worse time for the American public and the US healthcare system.
At the precise moment when the nation needs clinical laboratories to begin performing millions of tests for SARS-CoV-2, the coronavirus that causes the COVID-19 illness, those same labs are watching their cash flow collapse.
Data from multiple sources gathered by The Dark Report, sister publication of Dark Daily, confirm that—beginning in early March and continuing through last week—clinical laboratories in the United States saw incoming flows of routine specimens decline by between 50% and 60%. During this same time, lab revenue fell by similar amounts.
Clinical Lab Industry Currently Losing $800 to $900 Million Weekly
To give this decline context, the healthcare system spends about $80 billion annually on medical laboratory testing. Thus, labs across the US generated about $1.5 billion in revenue each week during 2019 and into 2020. By April 5, the decline in routine lab specimen volumes reached 55% to 60%. Since then, the clinical lab industry now loses between $800 million and $900 million each week. Total revenue loss from previous levels is already estimated to be $5.2 billion, and it is growing by an additional $800 million to $900 million every week that patients stay away from hospitals and physicians’ offices.
In the eight weeks since the COVID-19 pandemic caused patients to cease coming to hospitals and visiting their doctors, incoming routine specimens and revenue fell by 60%, causing cumulative lost routine revenue of $5.2 billion for the clinical laboratory industry in the United States. Each week that the existing shelter-in-place directives are effective, labs lose another $800 million to $900 million. The Dark Report based these estimates on data provided by multiple companies working with lab billing/claims, middleware analytical solutions, and customer relationship management (CRM) and electronic health record (EHR) products. (Chart copyright: The Dark Intelligence Group, Inc.)
The recent dire financial condition of labs small and large has gone unremarked by federal healthcare officials at the daily White House COVID-19 Task Force briefings. National news sources have yet to report on this development and its implications for successfully expanding the availability and numbers of COVID-19 tests in response to the pandemic.
The rapid and deep decline in specimens and revenue is not limited to clinical laboratories. Biopsy cases referred to anatomic pathology groups have declined by 50% to 60%. Some subspecialty pathology labs saw case referrals drop by 80% or more.
The nation’s two biggest clinical laboratory companies confirmed similar declines in their normal daily flow of routine specimens. Both companies recently reported first-quarter earnings (which included the month of March).
Quest Diagnostics, LabCorp Each Disclose Volume Declines of 50% to 60%
During its Q1 2020 earnings conference call, Chairman, President, and CEO of Quest Diagnostics (NYSE:DGX), Steve Rusckowski, stated, “In April, volume declines continue to intensify as we are seeing signs that volume declines are bottoming out at around 50% to 60%.”
The drop-off in routine lab test referrals was the similar at LabCorp (NYSE:LH). “In our diagnostics business, at the end of the quarter, we experienced reductions in demand for testing of 50% to 55% versus the company’s normal daily levels,” explained Glenn Eisenberg, Executive Vice President and CFO during LabCorp’s Q1 2020 earnings call. “This reduction in demand impacted testing volume broadly but was more heavily weighted towards routine procedures.”
Interviews with independent clinical lab owners and the administrative directors of hospital and health system labs further confirm this rapid and dramatic decline in the number of routine specimens arriving in their labs. Fewer specimens mean fewer claims, which means less revenue to laboratories.
Two Different Financial Futures for ‘Have’ Labs and ‘Have Not’ Labs
What happens next to the clinical laboratory industry in the United States—and to its ability to continue ramping up the availability of adequate numbers of COVID-19 tests in major cities, small towns, and rural areas—will be a story of “haves” and “have nots.”
The “haves” are clinical labs that have access to money. These are publicly-traded lab companies, academic medical center labs, and the sophisticated labs of health networks that operate multiple hospitals. In each case, these organizations have capital reserves and access to loans that will probably enable them to sustain COVID-19 lab testing services at the large volumes required to respond to the pandemic.
clinical labs operated by community hospitals and rural hospitals that were not financially robust before the onset of the pandemic; and,
specialty lab companies that perform a specific number of proprietary diagnostic tests (and for which demand has collapsed as patients stopped seeing their doctors).
Medicare Led Payers in the ‘Lab Test Price Race to the Bottom’
Prior to the onset of the SARS-CoV-2 pandemic, the finances of the “have-not” labs were already shaky, with many on the verge of filing bankruptcy, closing, or selling to a bigger lab company. Much blame for the deteriorating finances at a large proportion of community lab companies, community hospital labs, and rural hospital labs can be attributed to the deep, multi-year price cuts to the Medicare Part B clinical laboratory fee schedule as mandated by the Protecting Access to Medicare Act of 2014 (PAMA).
Medicare’s multi-year cuts to lab test prices were immediately copied by most state Medicaid programs. During this period, private payers followed Medicare’s lead and enacted their own deep cuts to the prices they paid labs for both routine tests and molecular/genetic tests.
That is why—when the pandemic intensified in early March—the 50% to 60% drop in specimens and revenue that hit these labs starved them of essential cash flow. When polled, the owners and directors of these labs acknowledge layoffs of the majority of their staff in all departments. They also reported substantial delays—both in submitted lab test claims and in getting payment for those claims—because claims-processing departments at the labs and private health insurers are understaffed due to shelter-in-place directives.
COVID-19 Test Revenue Helps Only Labs Performing Those Tests
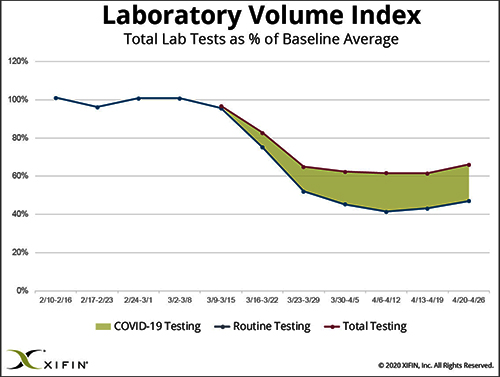
Revenue from COVID-19 testing is helping certain labs offset the revenue loss from fewer routine specimens. XIFIN, Inc., a San Diego company that provides revenue cycle management (RCM) services for clinical laboratories and pathology groups, analyzed the lab test claims for COVID-19 rapid molecular tests. It determined that labs performing these tests are generating enough revenue from these test claims to equal about 20% of their pre-pandemic revenue.
The chart above was prepared by XIFIN, Inc., of San Diego and is based on the changes XIFIN observed in the volume of routine clinical laboratory test claims generated by client labs on a weekly basis. In the first two months of 2020, routine lab test claims ran at expected levels until the first week of March. During the rest of March, routine lab test claims declined by 60%. During April, incoming routine lab test claims remained 55% to 60% below pre-pandemic levels. The shaded area shows the number of COVID-19 test claims coming into clinical labs. XIFIN says COVID-19 test claims make up about 20% of the decline in routine test specimens for those labs performing COVID-19 tests. The Dark Report estimates that the clinical laboratory industry has lost $800 million to $900 million in routine test revenue each week since March 23. Weekly revenue losses will continue at this rate until patients begin visiting their physicians and hospitals again perform elective services. (Chart copyright: XIFIN, Inc.)
Many CLIA-certified community laboratories and hospital labs have the diagnostic instruments and experience to perform rapid molecular tests for COVID-19. But when contacted, they tell us that their suppliers do not ship them even minimal quantities of the COVID-19 kits, the reagents, and the consumables. Thus, they cannot meet the needs of their client physicians. Instead, they watch as these physicians refer COVID-19 tests to the nation’s largest labs. The supply shortage prevents these smaller labs from doing larger numbers of COVID-19 test for the patients in the communities they serve. It also prevents them from earning the revenues from COVID-19 testing that currently helps the nation’s “have” labs offset the decline in revenue from routine testing.
Congress, national healthcare policymakers, and state governors need to immediately address this situation. Each week that passes during the COVID-19 pandemic and the shelter-in-place directives drains another $800 million to $900 million in revenue from routine lab testing that previously flowed into the nation’s clinical laboratories.
‘Have-not’ Clinical Labs in Small Towns Will Quietly Shrink and Disappear
Without timely intervention and financial support, the nation’s network of ‘have not’ labs, which have so capably served towns away from big metropolitan centers and rural areas, will quietly begin shrinking. One at a time, labs in small towns will close or sell. Local lab facilities will be shuttered and specimens from small-town patients will be transported to big labs hundreds or thousands of miles away.
It is also true that the financial disaster besetting the nation’s clinical laboratory industry will have comparable dramatic consequences for the in vitro diagnostics (IVD) manufacturers that sell them automation, analyzers, reagents, and other supplies. Since early March, IVD manufacturers watched as the pandemic caused orders for new instruments to collapse. During these same weeks, their clinical lab customers ceased ordering routine test kits at pre-pandemic levels. Dark Daily will cover the challenges confronting the IVD and other diagnostics industries in future e-briefings.
Announcing Free COVID-19 STAT Intelligence Briefings for Clinical Labs
With the COVID-19 pandemic creating chaos in nearly every aspect of healthcare, business, and society, clinical labs and their suppliers need timely intelligence and analysis about the innovations and successes achieved by their peers. This week, Dark Daily and The Dark Report are launching COVID-19 STAT Intelligence Briefings (Copy and paste this URL into your browser: https://www.covid19briefings.com). This comprehensive service is free and will cover four basic areas of needs for clinical laboratories as they ramp up COVID-19 testing:
Daily and weekly COVID-19 testing dashboards to guide every lab’s short-term planning;
Proven steps for labs to introduce and validate COVID-19 tests (both rapid molecular tests and serology tests);
Getting paid for COVID-19 testing to ensure every lab’s financial stability and clinical quality; and
Legal and regulatory updates for labs doing COVID19 tests to ensure full compliance.
Also, to help clinical laboratory leaders deal with the coming wave of COVID-19 serology tests, we are producing a free webinar led by James O. Westgard, PhD, FACB, and Sten Westgard, Director of Client Services and Technology, of Westgard QC, Inc.
Each week that the SARS-CoV-2 pandemic continues, and strict shelter-in-place directives are in place, the clinical laboratory industry loses another almost $900 million in revenue from lower volumes of routine testing. No industry can survive when its incoming revenue collapses by 50% to 60% for sustained periods of time.
Will Congress Recognize the Need for a Financial Rescue of ‘Have-not’ Labs?
Thus, it is incumbent on Congress, elected officials, and healthcare policymakers to recognize the financial consequences of the pandemic to the nation’s clinical laboratories. That is particularly true of the ‘have-not’ clinical labs. They do not have the same access to decisionmakers in government as billion-dollar lab companies.
And yet, these labs located in small communities and rural areas often are the only local labs that can do STAT testing in a couple of hours, and where clinical pathologists are personally familiar with local physicians and patients.
These “have-not” labs are vital healthcare resources. They should receive the help they need to get through this unprecedented crisis that is the COVID-19 pandemic.
Following criticism over delays in authorizing medical LDT COVID-19 tests, the FDA swiftly shut down consumer at-home specimen collection schemes
Banning COVID-19 tests that
rely on consumers’ collecting their own specimens at home is one example where
the federal US
Food and Drug Administration (FDA) took remarkably swift action. It’s also
interesting to note how some business people—who lack formal training in clinical
laboratory medicine—often are ready to seize any opportunity to sell lab
tests directly to consumers, regardless of whether such tests are reliable,
accurate, medically-necessary, and reasonably priced.
Last month, in the midst of this novel coronavirus
pandemic, the attempt by a handful of direct-to-consumer
(DTC) lab companies to sell COVID-19 tests to customers was speedily stopped by
the FDA less than 10 days after the agency became aware of the DTC testing
schemes. This all happened off the radar screen of most pathologists
and clinical laboratory administrators, whose full-time attention has been on
serving the urgent needs of their parent hospitals, referring physicians, and
patients.
Within days of each other, several direct-to-consumer lab
testing companies announced plans to offer COVID-19 tests to consumers. A
common feature of these offerings was that each DTC company would send a
collection kit to the consumer, who would collect his or her specimen at home.
The kit would then be sent to one of the DTC company’s CLIA-certified
laboratories, where the SARS-CoV-2
(Severe Acute Respiratory Syndrome Coronavirus 2) test would be performed.
A flurry of press releases and news interviews about how
consumers could order and pay for their own COVID-19 test, collect the specimen
at home, and have a Clinical
Laboratory Improvement Amendments (CLIA)-certified lab perform the test
quickly caught the attention of the FDA. Federal officials took immediate
action, or close to it.
On March 20, the FDA issued a warning to healthcare
consumers to beware of “unauthorized fraudulent COVID-19 test kits.” On the
same day, the FDA announced updated
guidance on its website pointing to recent policy adjustments stating
that “testing by CLIA-certified labs that had not yet acquired Emergency Use
Authorization (EUA) for their COVID-19 diagnostic does not apply to at-home
COVID-19 testing, ‘including self-collection of samples to be sent to a
clinical laboratory,’” reported MobiHealthNews.
“We want to alert the American public that, at this time,
the FDA has not authorized any test that is available to purchase for testing
yourself at home for COVID-19,” the FDA said in a
statement. “The FDA sees the public health value in expanding the
availability of COVID-19 testing through safe and accurate tests that may
include home collection, and we are actively working with test developers in
this space.”
Nevertheless, the FDA stipulated that at-home specimen
collection was still not authorized.
Collectively, the FDA’s two actions sent an unmistakable
message to the DTC lab companies that affected their consumer COVID-19 testing
plans. Following public release of the FDA’s recommendation and policy change,
several of the DTC lab companies posted messages on their websites disclosing
that they would not be selling COVID-19 tests with consumer self-collection
after all.
Everlywell Health’s DTC Clinical Laboratory Test Plan
News stories about the plans of these companies contained
details that pathologists and clinical laboratory managers will find
interesting. That is certainly true of Everlywell,
a DTC lab company with a distinctive background.
Austin-based Everlywell was founded in 2015 by Julia Cheek. She
appeared on the Shark
Tank television program in 2017 and received $1 million in funding for her
business plan, which Dark
Daily covered. Cheek’s plan was to sell selected medical laboratory
tests directly to consumers, including placing collection kits in retail stores
and pharmacies. in the same year, investors pumped another $4 million into Everlywell,
for a total of $5 million in venture capital funding, reported Business
Wire.
“The extreme shortage of tests for COVID-19 puts millions of Americans at risk,” said Julia Cheek (above), Founder and CEO of Everlywell, in a March 18, 2020, press release. She added, “Everlywell is committed to helping stop the spread of COVID-19 in the US by making this test widely available. As the national leader in at-home lab testing, we want to use our resources and expertise to help as many people as we can. We are committed to this fight, and we’re here to help.” A few days later, the FDA reiterated its ban on at-home COVID-19 specimen collection. (Photo copyright: Forbes/Whitney Martin.)
Everlywell, which manufactures laboratory test kits for
everything from general wellness and energy/weight, to men’s health, women’s
health, and sexual health, was among several companies that just days before
the FDA’s warning had announced plans for an at-home COVID-19 lab test with telehealth diagnosis.
Before the FDA banned at-home testing, Everlywell had an
initial supply of 30,000 collection kits and planned to work with “multiple
labs to scale infrastructure,” with a goal of testing 250,000 people weekly, stated
a company news
release. In news interviews, Everlywell said these consumer-collected
specimens would be done by CLIA-certified clinical laboratories. However, the
company did not name the lab companies it expected to use to perform those
tests.
Everlywell’s at-home test carried a $135 price tag for
consumers, an amount the company noted was “at-cost.” Before purchasing a
COVID-19 test, consumers are required to complete an eligibility questionnaire
developed in accordance with CDC recommendations. Testing includes a free telehealth
consultation with a board-certified physician for consumers who tested
positive.
However, after the FDA issued its March 20 warning, Everlywell
announced on its
website that its COVID-19 test would not be available for individual
purchase.
“Our frontline healthcare workers are in desperate need of
testing,” the site states. “We have made the decision to allocate today’s test
supply to hospitals and healthcare providers only.”
Everlywell was asked to comment on these matters by Dark Daily’s sister publication, The Dark Report. As of this date, the company has not responded to that request.
Other DTC Companies Suspend Plans to Sell At-Home
COVID-19 Test Kits
The Wall
Street Journal (WSJ) reported that Scanwell Health, Nurx Inc.,
and Curative Inc. also were among the handful of companies that curtailed plans
to launch at-home COVID-19 testing following the FDA’s announcement.
Scanwell Health now plans to wait for FDA clearance under
the EUA for its at-home COVID-19 blood test.
Though the US is making strides to increase testing, lack of
testing capacity has hamstrung the nation’s healthcare system as it attempts to
control the COVID-19 pandemic.
An at-home test would appear to be one option for increasing
COVID-19 testing nationwide. However, the FDA is signaling to these
direct-to-consumer lab testing companies—along with clinical laboratories—that
specimen quality issues associated with consumers collecting their own samples
carry the risk of producing inaccurate test results.
This is something that pathologists and medical laboratory
professionals understand because the largest source of errors in clinical
laboratory testing come from the pre-analytical stage. This is the part of the
testing process where a specimen is collected, then transported to a laboratory
and prepared for analysis at the bench.
First used to track cryptocurrencies such as Bitcoin, blockchain is finding its way into tracking and quality control systems in healthcare, including clinical laboratories and big pharma
Four companies were selected by the US Food and Drug Administration (FDA) to participate in a pilot program that will utilize blockchain technology to create a real-time monitoring network for pharmaceutical products. The companies selected by the FDA include: IBM (NYSE:IBM), Merck (NYSE:MRK), Walmart (NYSE:WMT), and KPMG, an international accounting firm. Each company will bring its own distinct expertise to the venture.
This important project to utilize blockchain technologies in
the pharmaceutical distribution chain is another example of prominent
healthcare organizations looking to benefit from blockchain technology.
Clinical laboratories and health insurers also are collaborating on blockchain projects. A recent intelligence briefing from The Dark Report, the sister publication of Dark Daily, describes collaborations between multiple health insurers and Quest Diagnostics to improve their provider directories using blockchain. (See, “Four Insurers, Quest Developing Blockchain,” July 1, 2019.)
Improving Traceability and Security in Healthcare
Blockchain continues to intrigue federal officials, health network administrators, and health information technology (HIT) developers looking for ways to accurately and efficiently track inventory, improve information access and retrieval, and increase the accuracy of collected and stored patient data.
In the FDA’s February press release announcing the pilot program, Scott Gottlieb, MD, who resigned as the FDA’s Commissioner in April, stated, “We’re invested in exploring new ways to improve traceability, in some cases using the same technologies that can enhance drug supply chain security, like the use of blockchain.”
Congress created this latest program, which is part of the federal US Drug Supply Chain Security Act (DSCSA) enacted in 2013, to identify and track certain prescription medications as they are disseminated nationwide. However, once fully tested, similar blockchain systems could be employed in all aspects of healthcare, including clinical laboratories, where critical supplies, fragile specimens, timing, and quality control are all present.
The FDA hopes the electronic framework being tested during
the pilot will help protect consumers from counterfeit, stolen, contaminated, or
harmful drugs, as well as:
reduce the time needed to track and trace
product inventory;
enable timely retrieval of accurate distribution
information;
increase the accuracy of data shared among the
network members; and
help maintain the integrity of products in the
distribution chain, including ensuring products are stored at the correct
temperature.
In the FDA’s February announcement, Scott Gottlieb, MD (above), the FDA Commissioner at that time, said, “For the drug track-and-trace system, our goals are to fully secure electronic product tracing, which provides a step-by-step account of where a drug product has been located and who has handled it, [and] establish a more robust product verification to ensure that a drug product is legitimate and unaltered.” It’s not hard to imagine how such a tracking system would be equally beneficial in clinical laboratories and hospital pathology departments. (Photo copyright: FDA.)
Companies in the FDA’s Blockchain Pilot
IBM, a leading blockchain provider, will serve as the
technology partner on the project. The tech giant has implemented and provided
blockchain applications to clients for years. Its cloud-based platform provides
customers with end-to-end capabilities that enable them to develop, maintain,
and secure their networks.
“Blockchain could provide an important new approach to further improving trust in the biopharmaceutical supply chain,” said Mark Treshock, Global Blockchain Solutions Leader for Healthcare and Life Sciences at IBM, in a news release. “We believe this is an ideal use for the technology because it can not only provide an audit trail that tracks drugs within the supply chain; it can track who has shared data and with whom, without revealing the data itself. Blockchain has the potential to transform how pharmaceutical data is controlled, managed, shared and acted upon throughout the lifetime history of a drug.”
Merck, known as MSD outside of the US and Canada, is
a global pharmaceutical company that researches and develops medications and
vaccines for both human and animal diseases. Merck delivers health solutions to
customers in more than 140 countries across the globe.
“Our supply chain strategy, planning and logistics are built around the customers and patients we serve,” said Craig Kennedy, Senior Vice President, Global Supply Chain Management at Merck, in the IBM news release. “Reliable and verifiable supply helps improve confidence among all the stakeholders—especially patients—while also strengthening the foundation of our business.”
Kennedy added that transparency is one of Merck’s primary
goals in participating in this blockchain project. “If you evaluate today’s
pharmaceutical supply chain system in the US, it’s really a series of handoffs
that are opaque to each other and owned by an individual party,” he said,
adding, “There is no transparency that provides end-to-end capabilities. This
hampers the ability for tracking and tracing within the supply chain.”
Walmart, the world’s largest company by revenue, will
be distributing drugs through their pharmacies and care clinics for the
project. Walmart has successfully experimented using blockchain technology with
other products. It hopes this new collaboration will benefit their customers,
as well.
“With successful blockchain pilots in pork, mangoes, and leafy greens that provide enhanced traceability, we are looking forward to the same success and transparency in the biopharmaceutical supply chain,” said Karim Bennis, Vice President of Strategic Planning of Health and Wellness at Walmart, in the IBM news release. “We believe we have to go further than offering great products that help our customers live better at everyday low prices. Our customers also need to know they can trust us to help ensure products are safe. This pilot, and US Drug Supply Chain Security Act requirements, will help us do just that.”
KPMG, a multi-national professional services network
based in the Netherlands, will be providing knowledge regarding compliance
issues to the venture.
“Blockchain’s innate ability within a private, permissioned
network to provide an ‘immutable record’ makes it a logical tool to deploy to
help address DSCSA compliance requirements,” said Arun Ghosh, US Blockchain
Leader at KPMG, in the IBM news release. “The ability to leverage existing
cloud infrastructure is making enterprise blockchain increasingly affordable
and adaptable, helping drug manufacturers, distributors, and dispensers meet
their patient safety and supply chain integrity goals.”
The FDA’s blockchain project is scheduled to be completed in
the fourth quarter of 2019, with the end results being published in a DSCSA
report. The participating organizations will evaluate the need for and plan any
future steps at that time.
Blockchain is a new and relatively untested technology
within the healthcare industry. However, projects like those supported by the
FDA may bring this technology to the forefront for healthcare organizations,
including clinical laboratories and pathology groups. Once proven, blockchain
technology could have significant benefits for patient data accuracy and
security.
For blood brothers Quest and LabCorp this is good news, since the two medical laboratory companies perform most of the testing for the biggest DTC genetic test developers
Should clinical laboratories be concerned about direct-to-consumer (DTC) genetic tests? Despite alerts from healthcare organizations about the accuracy of DTC genetic testing—as well as calls from privacy organizations to give DTC customers more control over the use of their genetic data—millions of people have already taken DTC tests to learn about their genetic ancestry. And millions more are expected to send samples of their saliva to commercial DTC companies in the near future.
This growing demand for at-home DTC tests does not appear to be subsiding. And since most of the genetic testing is completed by the two largest lab companies—Quest Diagnostics (NYSE:DGX) and Laboratory Corporation of America (NYSE:LH)—other medical laboratories have yet to find their niche in the DTC industry.
Another factor is the recent FDA authorization allowing DTC company 23andme to report the results of its pharmacogenetic (PGx) test directly to customers without requiring a doctor’s order. For these reasons, this trend looks to be gaining momentum and support from federal governing organizations.
Dark Daily has
reported on DTC genetic
testing for many years. According to MIT’s Technology Review, 26 million people—roughly
8% of the US population—have already taken at-home DNA tests. And that number
is expected to balloon to more than 100 million in the next 24 months!
“The genetic genie is out of the bottle. And it’s not going
back,” Technology Review reports.
The vast majority of the genetic information gathered goes into the databases of just four companies, with the top two—Ancestry and 23andMe—leading by a wide margin. The other two major players are FamilyTreeDNA and MyHeritage, however, Ancestry and 23andMe have heavily invested in online and television advertising, which is paying off.
In an op-ed response to a NYT editorial that warned readers to avoid 23andMe’s DTC genetic testing, 23andMe CEO and co-founder Anne Wojcicki (above) wrote, “We believe that consumers can learn about genetic information without the help of a medical professional, and we have the data to support that claim.” The FDA agreed and in February approved 23andMe to report pharmacogenetic test results directly to its customers. How this will play out for clinical laboratories remains to be seen. (Photo copyright: Inc.com.)
As more people add their data to a given database, the likelihood they will find connections within that database increases. This is called the Network Effect (aka, demand-side economies of scale) and social media platforms grow in a similar manner. Because Ancestry and 23andMe have massive databases, they have more information and can make more connections for their customers. This has made it increasingly difficult for other companies to compete.
Quest Diagnostics and LabCorp do the actual gene sequencing
for the top players in the DTC genetic testing sector. The expected wave of new
DTC genetic test costumers (74 million in the next 24 months) will certainly
have a beneficial revenue impact on those two lab companies.
Why the Explosion in Genetic
Testing by Consumers?
In 2013, just over 100,000 people took tests to have their
DNA analyzed, mostly using Ancestry’s test, as Dark Daily reported. By 2017, that
number had risen to around 12 million, and though Ancestry still had the
majority market share, 23andMe was clearly becoming a force in the industry,
noted Technology Review.
And now there are several health-related reasons as well. For
example, the study of pharmacogenetics has led clinicians to understand that
certain genes reveal how our bodies process some medications. The FDA’s clearance
allows 23andMe to directly inform customers about “genetic variants that may be
associated with a patient’s ability to metabolize some medications to help
inform discussions with a healthcare provider. The FDA is authorizing the test
to detect 33 variants for multiple genes,” the FDA’s press
release noted.
Controversy Over DTC
Genetic Tests
The use of DTC genetic tests for healthcare purposes is not without scrutiny by regulatory agencies. The FDA removed 23andMe’s original health test from the market in 2013. According to Technology Review, the FDA’s letter was “one of the angriest ever sent to a private company” and said “that the company’s gene predictions were inaccurate and dangerous for those who might not fully understand the results.”
23andMe continues to refine its DTC tests. However, the debate continues. In February of this year, the New York Times (NYT) editorial board published an op-ed warning consumers to be wary of health tests offered by 23andMe, saying the tests “look for only a handful of [genetic] errors that may or may not elevate your risk of developing the disease in question. And they don’t factor into their final analysis other information, like family history.”
Anne Wojcicki, CEO and co-founder of 23andMe, responded with her own op-ed to the NYT, titled, “23andMe Responds: Empowering Consumers.” In her letter, Wojcicki contends that people should be empowered to take control of their own health, and that 23andMe allows them to do just that. “While 23andMe is not a diagnostic test for individuals with a strong family history of disease, it is a powerful and accurate screening tool that allows people to learn about themselves and some for the most common clinically useful genetic conditions,” she wrote.
Nevertheless, privacy concerns remain:
Who owns the results, the company or the
consumer?
Who can access them?
What happens to them a year or five years after
the test is taken?
When they are sold or used, are consumers
informed?
Even as experts question the accuracy of DTC genetic testing
in a healthcare context, and privacy concerns continue to grow, more people
each year are ordering the tests. With predictions of 74 million more tests
expected in the next 24 months, it’s certain that the medical laboratories that
process those tests will benefit.