Goal of his foundation is to provide access to COVID-19 medical laboratory tests for first responders, as well as low-cost tests to the general public
Early in April, when many of the nation’s clinical laboratories were facing numerous challenges in their attempts to obtain adequate supplies for collecting, transporting, and testing for COVID-19, a Hollywood actor was funding his foundation and obtaining enough supplies for his foundation to offer access to COVID-19 testing to residents in his community of Malibu—as well as in other areas.
In many ways, local medical laboratories that offer COVID-19 tests are competing with actor/philanthropist Sean Penn’s Community Organized Relief Effort (CORE) foundation for the supplies they need to provide COVID-19 testing to the patients in their own communities. The non-profit organization says it is working with various healthcare providers to provide free coronavirus testing to first responders, and low-cost testing to the general public, in eleven cities and counties in California, Georgia, North Carolina, and Illinois.
In fact, the volume of COVID-19 testing CORE currently provides is large enough that The Hollywood Report published a story on June 3, titled, “How Sean Penn Made the Biggest COVID-19 Testing Site in U.S.” The article stated that, “In late May, Mayor Eric Garcetti announced the opening of a new COVID-19 testing site at Dodger Stadium in partnership with CORE, the Los Angeles Dodgers, Live Nation Entertainment, Red Rock Entertainment, and the Los Angeles Fire Department. Operated by CORE and LAFD, this site has capacity to test 6,000 residents a day free of charge––making it three times the size of any other location in L.A. County and said to be the largest testing site in the U.S.”
The Reporter did not make the distinction that the Dodger Stadium site is only collecting specimens. And, no news accounts of the CORE COVID-19 testing program names the clinical laboratories that CORE currently uses to perform the coronavirus tests for the specimens it collects.
CORE Partnered with Private Healthcare Provider Elevated Health
CORE first got underway in 2010 providing disaster relief following the catastrophic magnitude 7.0 earthquake in Haiti. It was known then as the Jenkins-Penn Haitian Relief Organization (J/P HRO). The foundation initiated its support of COVID-19 testing efforts in California in April, reported the Orange County Register (OCR). At that time, testing was much more limited than it is today and drive-thru testing in most areas in America was not available.
Elevated Health’s COVID Clinic website enables consumers to complete pre-test enrollment and payment before arriving at the drive-up testing site at the Westminster Mall.
“Right now, hospitals have very strict guidelines on who can be tested. Public health departments are overwhelmed and possibly underfunded. That’s where I’m trying to bridge the gap,” Matthew Abinante, DO, a doctor of osteopathy and Elevated Health’s founder and CEO, told the OCR.
The coronavirus test kits Elevated Health uses are made in China and were purchased from Georgia-based HealthTrackRx. According to Abinante, they are “FDA authorized, but not FDA approved,” reported the OCR.
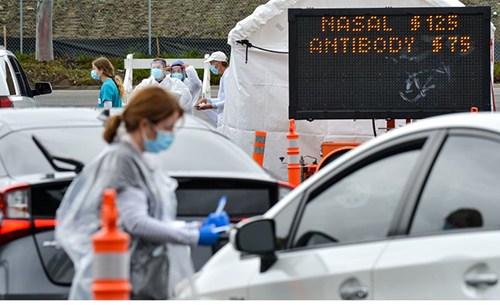
Clinical laboratory leaders may be intrigued to see consumers waiting their turn at drive-through testing lines as they take COVID-19 diagnosis into their own hands. Sites like the one above run by Elevated Health at the Westminster Mall demonstrate that people are willing to patronize providers that serve their needs directly. (Photo copyright: Orange County Register.)
CORE Aims to Be a Model for Partnering in Testing
Though CORE’s COVID-19 testing relief efforts are no longer limited to Los Angeles County, that is where it all began. Specimen collection at drive-through sites for COVID-19 tests initially prioritized first responders and essential workers. CORE funds provided for a staff of 70 people at four of the 35 drive-thru specimen collection sites in LA, reported CBS Los Angeles(CBSLA).
CORE-funded services also made it possible for Los Angeles city employees—who were running the drive-thru specimen collection sites—to return to their primary jobs as emergency first responders, reported the Associated Press (AP).
“It’s something that we can adapt to very quickly with the training of the Los Angeles Fire Department initially. And we’re able to take all those firemen and put them back in to serve the people in the way that we need them to,” said Penn in the AP article.
At that time, city officials planned to perform 10,000 tests a day, Deputy Mayor Jeff Gorell, JD, told the LA Times. The City of Los Angeles purchased the tests and CORE covered the cost of staff, volunteers, and personal protective equipment (PPE), reported the LA Times.
“We have servers and people from the Peace Corps, actresses—a lot of people from the communities where the test site is. We’re trying to hire as much locally as possible,” Ann Lee, CORE’s Chief Executive Officer, told Business Insider.
CORE also partnered with the City of Malibu in western Los Angeles County to provide mobile COVID-19 testing services for the city’s 3,000 residents, first responders, and essential workers from April 6 to 17 at a testing site at Malibu City Hall.
“This is what I hope will be a model in terms of the government and community foundation partnerships that can be replicated not only in the city of Los Angeles and throughout California, but throughout the country,” Sean Penn (above at the COVID-19 drive-thru testing site in Malibu, Calif.), founder of CORE, told CBSLA. Since making that statement, CORE has gone on to partner with healthcare providers in three other states to provide coronavirus drive-thru specimen collection. (Photo copyright: Associated Press/ABC News.)
Should Drive-Through Testing Continue Post-Pandemic?
An April Dark Daily e-briefing reported on drive-thru COVID-19 specimen collection operations across 30 states. The e-briefing also noted that drive-thru collections protects medical laboratory professionals and emergency department staff from possible exposure to infectious agents.
It’s likely many industries—from education and retail to travel and restaurants—will be revamped as a result of the pandemic. Clinical laboratory leaders and pathologists will want to study the different approaches used to develop drive-through COVID-19 specimen collection; how some providers that ran them partnered with charitable organizations such as CORE; why drive-thru specimen collection appeals to consumers; and how it may improve phlebotomists’ safety and increase clinical laboratory business.
Facing a backlog, the state’s public health laboratory turned to the medical laboratory at Dartmouth Hitchcock Medical Center
Much of the attention surrounding the COVID-19
outbreak—the illness caused by the SARS-CoV-2
coronavirus—has focused on large urban areas such as New York City and Los
Angeles. However, the virus is impacting many rural areas as well. This is true
in New Hampshire, where the diagnostic response required close cooperation
between the state’s public health
laboratory and the clinical
laboratory at its lone academic medical center. Their experience offers
lessons for medical
laboratory leaders nationwide.
“When these things happen and you surge beyond what you
could imagine, it’s the relationships with people that matter more than
anything,” said Christine
L. Bean, PhD, Administrator of New
Hampshire Public Health Laboratory Division of Public Health Services , Concord,
N.H., during a recent Dark
Daily webinar, titled, “What Hospital and Health System Labs Need to
Know About Operational Support and Logistics During the COVID-19 Outbreak.”
As Bean explained, during the earliest stages of the
pandemic the “CDC was doing the testing” and the state lab’s role was limited
to submitting samples from patients deemed as “presumptive positives.” Then, on
Feb. 4, the FDA granted an emergency
use authorization (EUA) allowing use of the CDC-developed real-time
reverse transcriptase PCR (RT-PCR) assay by designated labs.
The New Hampshire Public Health Laboratory (NHPHL) received
its first test kit on Feb. 10, Bean said. But the kits were recalled due to
validation problems with one of the reagents. On Feb. 26, the CDC
issued revised test instructions allowing use of the test without the N3
primer and probe set that had caused the early validation issues. The NHPHL
verified the test under the new guidelines and went live on March 2, she said.
However, with a capacity of 150 to 200 tests per day, the
lab wasn’t equipped to handle a large volume. “Much of what we do is really
population-based,” she said. “Most of the time we’re not doing patient
diagnostic testing.”
Christine L. Bean, PhD (left), Administrator of the New Hampshire Public Health Laboratory, and Joel Lefferts, PhD (right), Assistant Professor of Pathology and Laboratory Medicine, and Assistant Director of the Molecular Pathology, at Dartmouth’s Geisel School of Medicine, spoke with Dark Daily’s Editor-in-Chief Robert Michel during a webinar on what hospital and health system labs need to know about operational support and logistics during the COVID-19 outbreak. The webinar can be freely downloaded by clicking here. (Photo copyright: Dark Daily.)
NHPHL Turns to the Medical Laboratory at DHMC-CGHT for
Help
The DHMC-CGHT lab began having its own discussions about
testing in the first week of February, said Joel
A. Lefferts, PhD, HCLD, DABCC, Assistant Professor of Pathology and
Laboratory Medicine and Assistant Director of Molecular Pathology at
Dartmouth’s Geisel School of
Medicine. They were unsure of how much need there would be, but “throughout
the month of February, we started exploring different testing options,” he said
during the Dark Daily webinar.
The Dartmouth-Hitchcock lab team began with the CDC test. However,
Lefferts noted that the initial FDA guidance was “somewhat restrictive” and required
specific RNA extraction
kits and real-time PCR instruments. “If our lab didn’t have the capability to
perform everything exactly as indicated, we would be running it off-label and
would have to possibly submit our own EUA submission to the FDA,” he explained.
Later, though, the FDA and CDC loosened those restrictions and the lab began testing with the CDC assay on March 18, using a Thermo Fisher ABI 7500Dx instrument, Lefferts said. According to Thermo Fisher’s website, the ABI 7500Dx “is a real-time nucleic acid amplification and five-color fluorescence detection system available for in vitro diagnostic use.”
However, Lefferts continued, “we only had one of these
7500Dx instruments, and it was a relatively manual and labor-intensive
process.” It allowed a maximum of 29 samples per run, he said, and took about
five hours to produce results.
Then, the FDA granted an EUA for Abbott’s
m2000 assay, which runs on the company’s m2000rt real-time PCR instrument.
“We were really excited, because we happened to have two of these systems in
our lab,” he said. “We quickly got on the phone and ordered some of these
kits.”
The DHMC-CGHT lab went live with the new system on March 23.
It can handle up to 94 samples per run, said Lefferts, and with two instruments
running from 6 a.m. to 9 p.m., “there’s a potential to do as many as 10 runs
per day.”
This was the system they used to help New Hampshire’s Public
Health Lab with its backlog. “It was unbelievable to see that our backlog could
be really wiped out,” said Bean.
Challenges for Medical Labs
Gearing up for testing in a public health emergency poses
many challenges, Lefferts advised. “You need to look at what instrumentation
you have in your laboratory, what the experience level of your lab team is, how
much space you have, your expected batch size, and your needed turnaround
time.”
The two labs also had to deal with regulatory uncertainty. “This EUA process is something for which we don’t have much experience,” he said. “Trying to juggle CLIA, CAP, the FDA, and possibly state regulations is a bit challenging. You definitely need to do your research and talk to other clinical laboratories that are doing this testing to get advice.”
Lefferts explained that the most significant challenges to
develop and validate a molecular assay for COVID-19 included:
Availability of validation materials.
Obtaining “positive [viral] samples may be a challenge, depending on where you
are and what you have access to,” said Lefferts. However, he credits the FDA
for being “very proactive” in suggesting alternative sources for “viral isolates or genomic RNA that’s been
extracted from some of these viral isolates.”
Availability of collection kits. “We can
do a lot more testing now,” he said, but one bottleneck is the limited
availability of supplies such as nasopharyngeal swabs
and viral transport media. “We’re looking at alternative collection options,”
he said, such as 3D-printed swabs or even Q-tips [household cotton swabs], though
“hopefully it won’t come to that.” The DHMC-CGHT lab also considered producing its
own transport media.
Turnaround times. “Our lab wants to get
those results out as soon as possible,” Lefferts said. “So, we’re looking at
alternative methods to get that testing out sooner.” For example, “do we just
do the SARS-CoV-2 testing on a patient, or do we need to do other influenza and other viral
pathogens,” while also keeping up with other routine testing during the
pandemic?
Staffing issues. “Fatigue is a big issue
with members of our labs who put in lots of extra hours,” he said. The
DHMC-CGHT lab has developed contingency plans in case lab personnel get sick.
This critical information will be highly useful for
Laboratory Directors and Managers, Laboratory Supervisors and Team Leaders,
Integrated Health System Leaders, Hospital Group Leaders, Physicians and
Physician Group Leaders, Phlebotomy Managers, Courier and Logistics Managers,
and Safety and Compliance Managers.
Using 3D printing and a chemical heat source, University of Pennsylvania researchers have created a proof-of-concept for an affordable Zika test that returns results in just 40 minutes
There’s a gap in Zika virus testing that researchers at the University of Pennsylvania hope to fill. That gap is a point-of-care test for the Zika virus that can produce a fast and accurate result, whether in developed nations or in developing countries that don’t have many state-of-the art clinical laboratories.