Molecular probes designed to spot minute amounts of pathogens in biological samples may aid clinical laboratories’ speed-to-answer
Driven to find a better way to isolate minute samples of pathogens from among high-volumes of other biological organisms, researchers at Canada’s McMaster University in Hamilton, Ontario, have unveiled a bioinformatics algorithm which they claim shortens time-to-answer and speeds diagnosis of deadly diseases.
Two disease pathogens the researchers specifically targeted in their study are responsible for sepsis and SARS-CoV-2, the coronavirus causing COVID-19. Clinical laboratories would welcome a technology which both shortens time-to-answer and improves diagnostic accuracy, particularly for pathogens such as sepsis and SARS-CoV-2.
Their design of molecular probes that target the genomic sequences of specific pathogens can enable diagnosticians and clinical laboratories to spot extremely small amounts of viral and bacterial pathogens in patients’ biological samples, as well as in the environment and wildlife.
“There are thousands of bacterial pathogens and being able to determine which one is present in a patient’s blood sample could lead to the correct treatment faster when time is very important,” Zachery Dickson, a lead author of the study, told Brighter World. Dickson is a bioinformatics PhD candidate in the Department of Biology at McMaster University. “The probe makes identification much faster, meaning we could potentially save people who might otherwise die,” he added.
Sepsis is a life-threatening response to infection that leads to organ failure, tissue damage, and death in hospitals worldwide. According to Sepsis Alliance, about 30% of people diagnosed with severe sepsis will die without quick and proper treatment. Thus, a “shortcut” to identifying sepsis in its early stages may well save many lives, the McMaster researchers noted.
And COVID-19 has killed millions. Such a tool that identifies sepsis and SARS-CoV-2 in minute biological samples would be a boon to hospital medical laboratories worldwide.
“We currently need faster, cheaper, and more succinct ways to detect pathogens in human and environmental samples that democratize the hunt, and this pipeline does exactly that,” Hendrik Poinar, PhD (above), McMaster Professor of Anthropology and a lead author of the study, told Brighter World. Poinar is Director of the McMaster University Ancient DNA Center. Hospital medical laboratories could help save many lives if sepsis and COVID-19 could be detected earlier. (Graphic copyright: McMaster University.)
Is Bioinformatics ‘Shortcut’ Faster than PCR Testing?
The researchers say their probes enable a shortcut to detection—even in an infection’s early stages—by “targeting, isolating, and identifying the DNA sequences specifically and simultaneously.”
The probes’ design makes possible simultaneous targeted capture of diverse metagenomics targets, Biocompare explained.
But is it faster than PCR (polymerase chain reaction) testing?
The McMaster scientists were motivated by the “challenges of low signal, high background, and uncertain targets that plague many metagenomic sequencing efforts,” they noted in their paper.
They pointed to challenges posed by PCR testing, a popular technique used for detection of sepsis pathogens as well as, more recently, for SARS-CoV-2, the coronavirus causing COVID-19.
“The (PCR) technique relies on primers that bind to nucleic acid sequences specific to an organism or group of organisms. Although capable of sensitive, rapid detection and quantification of a particular target, PCR is limited when multiple loci are targeted by primers,” the researchers wrote in Cell Reports Methods.
According to LabMedica, “A wide array of metagenomic study efforts are hampered by the same challenge: low concentrations of targets of interest combined with overwhelming amounts of background signal. Although PCR or naive DNA capture can be used when there are a small number of organisms of interest, design challenges become untenable for large numbers of targets.”
Detecting Pathogens Faster, Cheaper, and More Accurately
As part of their study, researchers tested two probe sets:
one to target bacterial pathogens linked to sepsis, and
another to detect coronaviruses including SARS-CoV-2.
They were successful in using the probes to capture a variety of pathogens linked to sepsis and SARS-CoV-2.
“We validated HUBDesign by generating probe sets targeting the breadth of coronavirus diversity, as well as a suite of bacterial pathogens often underlying sepsis. In separate experiments demonstrating significant, simultaneous enrichment, we captured SARS-CoV-2 and HCoV-NL63 [Human coronavirus NL 63] in a human RNA background and seven bacterial strains in human blood. HUBDesign has broad applicability wherever there are multiple organisms of interest,” the researchers wrote in Cell Reports Methods.
The findings also have implications to the environment and wildlife, the researchers noted.
Of course, more research is needed to validate the tool’s usefulness in medical diagnostics. The McMaster University researchers intend to improve HUBDesign’s efficiency but note that probes cannot be designed for unknown targets.
Nevertheless, the advanced application of novel technologies to diagnose of sepsis, which causes 250,000 deaths in the US each year, according to the federal Centers for Disease Control and Prevention, is a positive development worth watching.
The McMaster scientists’ discoveries—confirmed by future research and clinical studies—could go a long way toward ending the dire effects of sepsis as well as COVID-19. That would be a welcome development, particularly for hospital-based laboratories.
The antibodies target portions of the SARS-CoV-2 spike protein that resist mutation, potentially leading to better treatments and vaccines
One challenge in the battle against COVID-19 is the emergence of SARS-CoV-2 variants, especially the Delta variant, which may be more resistant to neutralizing antibodies compared with the original coronavirus. But now, scientists led by researchers at the Fred Hutchinson Cancer Research Center (Fred Hutch) in Seattle say they have identified antibodies that could be broadly protective against multiple sarbecoviruses, the subgenus that contains SARS-CoV-2 as well as SARS-CoV-1, the virus responsible for the 2002-2004 severe acute respiratory syndrome (SARS) outbreak.
In “SARS-CoV-2 RBD Antibodies That Maximize Breadth and Resistance to Escape,” the researchers described how they compared 12 antibodies obtained from patients infected with either SARS-CoV-2 or SARS-CoV-1. They pointed to one antibody in particular—S2H97—that could lead to development of new vaccines and therapies against current and future variants. It might even protect against sarbecoviruses that have not yet been identified, they wrote.
Unsaid in the news release about these research findings is the fact that these particular antibodies could eventually become useful biomarkers for clinical laboratory tests designed to help physicians determine which patients have these antibodies—and the protection from infection they represent—and which do not.
So far, however, S2H97 has only been tested in hamsters. But results are promising.
“This antibody, which binds to a previously unknown site on the coronavirus spike protein, appears to neutralize all known sarbecoviruses—the genus of coronaviruses that cause respiratory infections in mammals,” said Jay Nix, PhD, an affiliate in Berkeley Lab’s Biosciences Area and Beamline Director of the Molecular Biology Consortium at Berkeley Lab’s Advanced Light Source (ALS), in a Berkeley Lab news release. “And, due to the unique binding site on mutation-resistant part of the virus, it may well be more difficult for a new strain to escape,” he added.
Scientists have long known that the SARS-CoV-2 virus uses the spike protein to attach to human cells. The federal Centers for Disease Control and Prevention (CDC) notes that the variants have mutations in their spike proteins that make some of them more transmissible.
The Delta variant, the CDC notes, was the predominant variant in the US as of August 28, 2021. It “has been shown to have increased transmissibility, potential reduction in neutralization by some monoclonal antibody treatments, and reduction in neutralization by post-vaccination sera,” the agency states.
The key to S2H97, the researchers wrote, is that it targets a portion of the spike protein that is common among sarbecoviruses, and that is likely to be resistant to mutations.
The researchers used a variety of techniques to analyze how the 12 antibodies bind to the virus. They “compiled a list of thousands of mutations in the binding domains of multiple SARS-CoV-2 variants,” Nature reported. “They also catalogued mutations in the binding domain on dozens of SARS-CoV-2-like coronaviruses that belong to a group called the sarbecoviruses. Finally, they assessed how all these mutations affect the 12 antibodies’ ability to stick to the binding domain.”
William Schaffner, MD (above), Professor of Preventive Medicine in the Department of Health Policy as well as Professor of Medicine in the Division of Infectious Diseases at the Vanderbilt University School of Medicine in Nashville, believes that “people who test positive for SARS-CoV-2 and who are at risk of progressing to severe disease—including those who are over the age of 65 years and those who have weakened immune systems—should talk with a doctor about receiving monoclonal antibody treatment,” Medical News Today reported. “[The monoclonal antibody treatment is] designed to prevent the evolution of the infection from a mild infection into a serious one,” he noted. “In other words, you’ve just [contracted the virus], but we can now give you a medication that will help prevent [you] being hospitalized and getting seriously ill.” (Photo copyright: Vanderbilt University.)
Earlier Antibody Treatment Receives an EUA from the FDA
In issuing the EUA for sotrovimab, the FDA cited “an interim analysis from a phase 1/2/3 randomized, double-blind, placebo-controlled clinical trial in 583 non-hospitalized adults with mild-to-moderate COVID-19 symptoms and a positive SARS-CoV-2 test result. Of these patients, 291 received sotrovimab and 292 received a placebo within five days of onset of COVID-19 symptoms.”
Among these patients, 21 in the placebo group were hospitalized or died compared with three who received the therapy, an 85% reduction.
“While preventive measures, including vaccines, can reduce the total number of cases, sotrovimab is an important treatment option for those who become ill with COVID-19 and are at high risk—allowing them to avoid hospitalization or worse,” stated Adrienne E. Shapiro, MD, PhD, of the Fred Hutchinson Cancer Research Center in a GSK news release. Shapiro was an investigator in the clinical trial.
The EUA allows use of sotrovimab in patients who have tested positive for SARS-CoV-2, have mild-to-moderate symptoms, and “who are at high risk for progression to severe COVID-19, including hospitalization or death. This includes, for example, individuals who are 65 years of age and older or individuals who have certain medical conditions.” It is not authorized for patients who are hospitalized or for those who require oxygen therapy.
The therapy was originally known as VIR-7831. The companies say they have developed a similar treatment, VIR-7832, with modifications designed to enhance T cell function against the disease.
The antibody, they wrote, targets a region of the SARS-CoV-1 spike protein that is “highly conserved” among sarbecoviruses. Clinical laboratory testing, they wrote, also indicated that the therapy was likely to be effective against known SARS-CoV-2 variants.
“Our distinctive scientific approach has led to a single monoclonal antibody that, based on an interim analysis, resulted in an 85% reduction in all-cause hospitalizations or death, and has demonstrated, in vitro, that it retains activity against all known variants of concern, including the emerging variant from India,” stated Vir Biotechnology CEO George Scangos, PhD, in the GSK news release. “I believe that sotrovimab is a critical new treatment option in the fight against the current pandemic and potentially for future coronavirus outbreaks, as well.”
Pathologists and clinical laboratory managers working with rapid molecular tests and antibody tests for COVID-19 will want to monitor the development of monoclonal antibody treatments, as well as further research studies that focus on these specific antibodies.
Intriguing technology may find immediate value in assisting the detection and tracking of COVID-19 worldwide
Pathologists and clinical laboratory personnel old enough to have watched Star Trek on television will recall the tricorder, a multi-functional handheld device that could non-invasively detect any disease or medical condition that the science fiction series needed to be revealed. Fiction, yes, but so was the Star Trekcommunicator before the advent of smartphones.
Now, Florida-based Advanced Medical Solutions International (AMSI) anticipates bringing to market in early 2022 a similar tricorder-like handheld device that detects SARS-CoV-2 in humans and on contaminated objects and surfaces.
AMSI’s COVID Hunter™ device would be the world’s first noninvasive touchless viral detector for COVID-19, which has reportedly killed 4.55 million people worldwide. The inventors make the point that the device is simply to detect the presence of the coronavirus. It is not a diagnostic test.
For clinical laboratory scientists, this is yet another example of new technology being applied to a clinical problem that could ultimately lead to new diagnostic tools, not only for COVID-19, but ultimately for other viruses as well.
Pictured above is the actual COVID Hunter™ device that was extensively used in testing around the world. According to AMSI, this breakthrough technology can immediately detect COVID-19 in a person’s throat, lungs, sinuses, and breath, or on skin or clothes. High-touch areas such as door handles, mobile phones, and desktops also could be routinely checked for the virus and sanitized, breaking the transmission chain. (Photo copyright: Advanced Medical Solutions International.)
According to the COVID Hunter™ website, the device’s proprietary detection method utilizes a US-patent-pending detection technology that was initially invented by Engineer Nassar Said, a partner and inventor at AMSI. The method for detecting SARS-CoV-2 (the coronavirus that causes COVID-19) utilizes the above patent-pending detection technology and was invented and developed by Nassar Said and Adeeb Al-Zoubi, PhD, immunologist, and AMSI co-founder and Chief Scientific Officer.
According to the inventors, the detection technology employed by the COVID Hunter™ utilizes a combination of radio frequency (RF) and infrared (IR) electromagnetic waves to detect the RNA and spike protein found in the SARS-CoV-2 coronavirus with greater than 99% specificity and 99% sensitivity from as far as six feet away.
Al-Zoubi described the groundbreaking technology in a January 2021 news conference introducing the device. “This patent-pending technology uses a unique combination of light waves and sound waves combined to hone in on specific physical, chemical, and biological characteristics of SARS-CoV-2,” he said.
“We are basically surrounding the virus and characterizing the virus on all its characteristics all at once,” he continued. “Through focused research and tireless work, we at AMSI and Stem Cells Arabia [a Jordanian scientific research company] analyzed and specified these physical, chemical, and biological characteristics of SARS-CoV-2 and used these characteristics as one single value to target the detection by the COVID Hunter™.
“The sum of these specific SARS-CoV-2 characteristics is not found in any other virus or any other targets and constitutes a unique thumbprint of the virus,” he added.
“The handheld COVID Hunter™ will revolutionize the way SARS-CoV-2 (including mutated strains) is detected, slowing the spread of the deadly virus, saving lives, and returning life to ‘normal’ in the near future,” said AMSI co-founder and CEO Donald Redman (above center), with technology inventor/AMSI partner Nassar Said (left) and AMSI co-founder/Chief Scientific Officer and COVID Hunter™ co-inventor Adeeb Al-Zoubi, PhD (right), in a news release.
The COVID Hunter™ introductory press conference noted:
The COVID Hunter™ showed 100% accuracy and 100% specificity to detect only SARS-CoV-2 positive samples, distinguishing COVID-19 from viruses such as SARS-CoV-1, MERS, Influenza, and HIV,
The COVID Hunter™ detected all PCR positive COVID-19 test samples among more than 4,000 nasal swabs.
When more than 1,000 human subjects were tested with both PCR testing and the COVID Hunter™, the device confirmed as positive all confirmed COVID-19 cases.
4.8% of PCR false negatives in human subjects were accurately detected by the COVID Hunter™ as COVID-19 positive, indicating superior sensitivity to PCR testing.
76 out 94 confirmed COVID-19 positive individuals were shown to be infective, meaning they could transmit the disease.
The COVID Hunter™ was able to track the mode of transmission of COVID-19 as the virus moved from hand to mouth to other people and objects. Developers found that a healthy individual who shook hands with an infected person could transmit the virus to a third party without becoming infected themselves.
Researchers detected COVID-19 on the feet of domestic pets, indicating pets could transmit the virus to multiple persons within a household.
Al-Zoubi said nine months of research and development resulted in several COVID Hunter™ prototypes that demonstrated accuracy, specificity, and sensitivity in experiments using both nasal swab samples and confirmed COVID-19 patients residing in quarantine areas and hospitals in different countries.
“I am excited to see the COVID Hunter™ go from the prototype phase to a fully refined manufactured device that can be used to save lives around the world,” Al-Zoubi said in his concluding remarks.
Mass Production of COVID-Hunter
In an exclusive interview with Dark Daily, Redman and Al-Zoubi said they are seeking additional investor backing so they can shift from product refinement to high-volume manufacturing. If funding is secured this fall, their goal is to begin production in January 2022 of up to 30,000 units per month, which are projected to sell for $3,000 per device. Initially, the COVID Hunter™ would be marketed only as a COVID-19 detection tool under Federal Trade Commission (FTC) regulations.
Once manufacturing begins, AMSI will be able to submit the required number of COVID Hunter™ devices to the federal Food and Drug Administration (FDA) for review, the final step in its application for Emergency Use Authorization (EUA) of the COVID Hunter™ as a COVID-19 diagnostic device. The company expects its expedited EUA review to be completed by early spring.
AMSI notes that COVID Hunter™ can perform up to 300 scans per hour and does not use consumables other than batteries. This, according to Al-Zoubi, makes it a game-changing device for the travel industry, schools, businesses, restaurants, professional sports franchises, and concert venues seeking a return to “normal” operations.
The COVID Hunter™ also will be capable of being updated online to precisely detect new virus mutations, making it a critical weapon to defeat the pandemic as new COVID-19 mutations are found.
“This device is highly tested and it’s much more accurate than PCR [testing] because it detects the virus based on the physical presence of the virus, not based on chemical reactions or antibodies,” Al-Zoubi told Dark Daily. “We have gone beyond proof-of-concept testing.”
Clinical pathologists will want to follow development of the COVID Hunter™ and see if it eventually receives FDA approval. It may fulfill its promise as a game-changing new technology, not just for detection, but also for diagnosis.
The inventors and developers of the COVID Hunter™ will present their technology and its potential uses in detection and diagnosis at the upcoming Executive War College on Laboratory and Pathology Management, which takes place at the San Antonio Hyatt Riverwalk Hotel on Nov. 2-3, 2021.
Adeeb Al-Zoubi, PhD, and Nassar Said will conduct the session titled “New Technology Preview: Meet the COVID Hunter™, a Non-Invasive, Touchless, Immediate, and Portable Detection Device That Identifies the SARS-Cov-2 Virus.”
Medical laboratory professionals interested in attending this informative presentation can register by clicking here or by copying https://www.executivewarcollege.com your browser.
Fear that immunity-resistant mutations of SARS-CoV-2 will emerge are real and the scientific community is paying close attention
Detection of an increasing number of new variants of the SARS-CoV-2 coronavirus raises the possibility that a new strain of COVID-19 might emerge that brings new problems to the management of the pandemic. Public health officials and clinical laboratory scientists are on the alert to determine if any new COVID-19 variant is more virulent or more easily transmissible.
Pathologists, along with the rest of the scientific community worldwide, are following reports of increasing coronavirus mutations with growing concern. The Alpha variant (Lineage B.1.1.7) accounted for most of the COVID-19 cases in April of 2021 in the US, though it was first identified in the United Kingdom. That was followed by the Iota variant (Lineage B.1.526) first identified in New York City. A series of other variants were to follow. Scientists were not surprised. It is normal for viruses to mutate, so they logged and tracked the mutations.
Then, the Delta variant (Lineage B.1.617.2) emerged during a severe outbreak in India. At first, it did not seem more threatening than any other variant, but that changed very quickly. Delta was different.
“The speed with which it dominated the pandemic has left scientists nervous about what the virus will do next. The variant battles of 2021 are part of a longer war, one that is far from over,” The Washington Post reported, which added, “Today, [Delta] has nearly wiped out all of its rivals. The coronavirus pandemic in America has become a Delta pandemic. By the end of July, it accounted for 93.4% of new infections, according to the Centers for Disease Control and Prevention.”
Why is Delta the Worst COVID-19 Variant So Far?
The Delta variant has two advantages that scientists know about:
Stickier spike protein than the spike on the original SARS-CoV-2 coronavirus, as well as on the other, earlier variants. This means that the Delta variant stands a better chance of remaining in a person’s nose or throat long enough to reproduce.
Faster replication. When a virus mutation has more opportunity to reproduce, it quickly becomes the main viral strain. This is the case with the Delta variant. Experts say that the viral load in patients with Delta is around 1,000 times higher than in patients with the original virus.
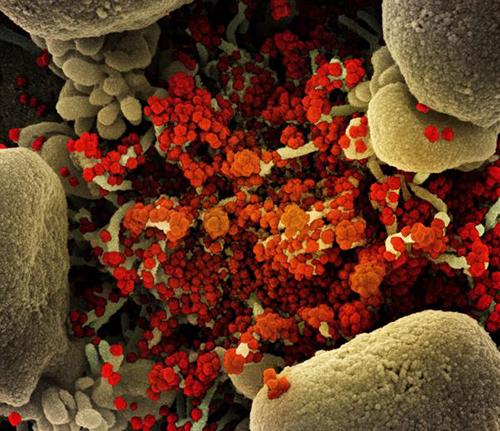
The image above is a “Colorized scanning electron micrograph of an apoptotic cell (tan) heavily infected with SARS-COV-2 virus particles (orange), isolated from a patient sample,” Newsweek reported. (Photo copyright: National Institute of Allergy and Infectious Diseases/Newsweek.)
Will More Dangerous SARS-CoV-2 Variants Appear?
“The great fear is that nature could spit out some new variant that completely saps the power of vaccines and upends the progress we’ve made against the pandemic. But to virologists and immunologists, such a possibility seems very unlikely,” STAT reported.
That is because, unlike Influenza, which is also a coronavirus, SARS-CoV-2 variants are not able to share genetic materials and recombine into deadlier variants. Thus, scientists are skeptical that a variant could appear and wipe out the progress made with vaccines and treatments.
One of the reasons the Flu vaccine changes every year is Influenza’s ability to recombine into variants that can evade immunity. Therefore, scientists are beginning to suspect that SARS-CoV-2, like the Flu, will likely be around for a while.
“I don’t think eradication is on the table. But I think we could come up with something that’s better than what we have for the flu,” Sharone Green, MD, Associate Professor of Medicine, Division of Infectious Diseases and Immunology and Infection Control Officer at University of Massachusetts Medical School, told Newsweek.
Limiting Infections and Replication
Several factors combined to create the COVID-19 pandemic. But SARS-CoV-2 was a novel coronavirus, meaning it was a new pathogen of a known virus. This meant every person on the planet was a potential host.
The situation now is different. Thanks to natural immunity, vaccines, and treatments that shorten the infection, the SARS-CoV-2 coronavirus has less chance to replicate.
“The pressure is there, but the opportunity is not. The virus has to replicate in order to mutate, but each virus doesn’t get many lottery tickets in a vaccinated person who’s infected,” Jeremy Kamil, PhD, Associate Professor of Microbiology and Immunology at LSU Health in Shreveport, La., told STAT.
Tracking Variants of Interest and Variants of Concern
The World Health Organization (WHO) has been monitoring the viral evolution of SARS-CoV-2 since the beginning of the pandemic. In late 2020, the WHO created categories for tracking variants:
VOIs are “A variant with specific genetic markers that have been associated with changes to receptor binding, reduced neutralization by antibodies generated against previous infection or vaccination, reduced efficacy of treatments, potential diagnostic impact, or predicted increase in transmissibility or disease severity.”
Current VOIs include:
Eta (Lineage B.1.525), detected in multiple countries, designated a VOI in March 2021.
Iota (Lineage B.1.526), US, first detected in November 2020, designated a VOI in March 2021.
Lambda (lineage C.37), Peru, first detected in December 2020, designated a VOI in June 2021.
VOCs, on the other hand, demonstrate all the characteristics of VOIs and also demonstrate “an increase in transmissibility, more severe disease (e.g., increased hospitalizations or deaths), significant reduction in neutralization by antibodies generated during previous infection or vaccination, reduced effectiveness of treatments or vaccines, or diagnostic detection failures.”
Current VOCs include:
Alpha (lineage B.1.1.7), first detected in the UK, September 2020.
Delta (lineage B.1.617.2), first detected in India, October 2020.
Will Vaccines Stop Working?
With each new variant, there tends to be a flurry of media attention and fearmongering. That a variant could emerge which would render our current vaccines ineffective has the scientific community’s attention.
“There is intense interest in whether mutations in the spike glycoprotein mediate escape from host antibodies and could potentially compromise vaccine effectiveness, since spike is the major viral antigen in the current vaccines,” wrote Adam S. Lauring, MD, PhD, and Emma B. Hodcroft, PhD, in “Genetic Variants of SARS-CoV-2—What Do They Mean?” published in the Journal of the American Medical Association (JAMA).
“Because current vaccines provoke an immune response to the entire spike protein, it is hoped that effective protection may still occur despite a few changes at antigenic sites in SARS-CoV-2 variants,” they added.
Future events may justify the optimism that the ongoing effectiveness of vaccines will help with many COVID-19 variants. But pathologists and clinical laboratory leaders may want to be vigilant, because as infection rates increase, so do workloads and demands on critical resources in their medical laboratories.
FDA cites ‘risk of false results’ and concerns about labeling and ‘performance claims’ in its official warning letter to Innova, a company with connections to Chinese firms
By many standards, the US government’s response to the COVID-19 pandemic has been phenomenal. However, the many emergency use authorizations (EUAs) awarded by the US federal Food and Drug Administration (FDA) to bring as many COVID-19 tests to market as quickly as possible means some of those tests in use today at clinical laboratories nationwide have not undergone the normal pre-market review and clearance typically required by the FDA.
But in its recall announcement, the FDA described Innova’s recall of its SARS-CoV-2 Antigen Rapid Test as a “Class 1 recall” and gave the stern warning, “Use of these devices may cause serious injuries or death.”
And in its public Safety Communication, the federal agency wrote, “The FDA has significant concerns that the performance of the test has not been adequately established, presenting a risk to health. In addition, labeling distributed with certain configurations of the test includes performance claims that did not accurately reflect the performance estimates observed during the clinical studies of the tests. Finally, the test has not been authorized, cleared, or approved by the FDA for commercial distribution or use in the United States, as required by law.”
In May 2021, Innova Medical Group of Pasadena, Calif., announced it would start producing millions of its COVID-19 SARS-CoV-2 Antigen Rapid test kits (above) per day in the United Kingdom by opening a production facility in Rhymney, South Wales. (Photo copyright: Innova Medical Group, Inc.)
FDA Warns Public to Stop Using Innova’s Rapid Antigen COVID-19 Test
Widescale COVID-19 testing has been viewed as key to containing community spread of the SARS-CoV-2 coronavirus, and fast, inexpensive rapid COVID-19 testing is a necessity in that fight.
However, as clinical laboratory scientists know, rapid tests are not as specific as molecular polymerase chain reaction (PCR) tests, which means there is a higher chance of false negatives and false positives with a COVID-19 rapid test than with a molecular test. When diagnosing COVID-19, a PCR test is considered the gold-standard, though results can take multiple days to produce.
Nevertheless, according to the Innova Europe website, the Innova rapid antigen test has a sensitivity on symptomatic individuals of 97% and a specificity of 99% and is the most widely used test in the world. More than 500 million units are in circulation.
Regardless, in its June 10th warning, the FDA called for the public to stop using the Innova Medical Group SARS-CoV-2 Antigen Rapid test for diagnostic use.
“The FDA has significant concerns that the performance of the test has not been adequately established, presenting a risk to health,” the FDA stated. “In addition, labeling distributed with certain configurations of the test includes performance claims that did not accurately reflect the performance estimates observed during the clinical studies of the tests. Finally, the test has not been authorized, cleared, or approved by the FDA for commercial distribution or use in the United States, as required by law.”
In its warning, the FDA recommended anyone in possession of Innova tests “destroy the tests by placing them in the trash” or return the tests to Innova.
The Innova SARS-CoV-2 Antigen Rapid test is also distributed under the names:
Innova COVID-19 Self-Test Kit (3T Configuration),
Innova Medical Group SARS-CoV-2-Antigen Rapid Test (7T Configuration), and
Innova Medical Group SARS-CoV-2-Antigen Rapid Test (25T Configuration).
Innova Medical Group was formed in March 2020 by Charles Huang, PhD, founder and chairman of private-equity firm Pasaca Capital. The Pasaca website states Innova worked with its primary contract manufacturer, China-based Xiamen Biotime Biotechnology Co., for several months to design “a highly accurate rapid antigen test for COVID-19.”
“The simple test takes less than five minutes to administer and generates results in as little as 20 minutes without the need for a machine,” the website states. “Equally important, Innova and its partner have been able to manufacture the product at scale, presently in excess of ten million kits per day.”
However, The Los Angeles Times claims that in September 2020 Innova “secured a vast supply of rapid coronavirus tests from an obscure Chinese manufacturer before established pharmaceutical companies could do so.” The LA Times adds that Innova distributed more than 70,000 tests in the United States even though the FDA had not acted on Innova’s application to sell its tests domestically.
This may have contributed to the FDA’s dire warning to discontinue use and discard the Innova tests.
UK’s MHRA Disagrees with FDA Warning
But in the UK, it is a different story. According to The Guardian, Innova’s lateral flow tests are the cornerstone of “Operation Moonshot”, the government’s mass testing plan aimed at reducing community transmission by identifying asymptomatic COVID-19 positive people using an inexpensive, quick-response test distributed for home use and to workplaces, schools, and test centers.
In “Rapid COVID Tests Used in Mass UK Programme Get Scathing US Report,” The Guardian reports that “criticism of the Innova test has been fierce” in the UK following the FDA’s “scathing review” of its rapid antigen test. However, after investigating the concerns raised by the FDA, the UK’s Medicines and Healthcare Products Regulatory Agency (MHRA) reiterated that the Innova lateral flow tests were safe to use.
“We have now concluded our review of the risk assessment and are satisfied that no further action is necessary or advisable at this time,” said Graeme Tunbridge, MHRA Director of Devices, in a UK government response statement which announced that the MHRA was extending the Exceptional Use Authorization (EUA) for the tests use in its national asymptomatic testing program through Aug. 28, 2021. “This has allowed us to extend the EUA to allow ongoing supply of these [lateral flow devices] over the coming months. People can be assured of the MHRA’s work to continuously monitor the tests in use; as is our standard process.”
Innova Defends Its Test, FDA Repeats Its Warning
An Innova spokesperson told The Guardian: “The Innova rapid antigen test has been widely used, studied, tested, scrutinized and analyzed with data supporting the efficacy of the test from the largest mass testing program out of the UK. Innova is confident about the quality of its product.”
However, the FDA maintains Innova’s COVID-19 lateral flow test included labeling that provided “false and misleading” estimates of the test’s clinical performance. In its warning letter to Innova, the FDA also pointed out that the clinical study data Innova submitted as part of its EUA request was “identical to data previously provided by other manufacturers in their EUA requests. The data reliability and accuracy issues noted herein raise significant concerns that the performance of the SARS-CoV-2 Antigen Rapid Qualitative Test has not been adequately established, and that the products distributed by Innova without FDA approval, clearance, or authorization could present a serious risk to the public health.”
Pathologists and clinical laboratory professionals in this country will want to watch carefully to see if efforts to increase regulatory scrutiny of diagnostic tests in the UK spills across the Atlantic.