Data was used to create a transmission map that tracked the spread of infections among school athletes and helped public health officials determine where best to disrupt exposure
Genomic sequencing played a major role in tracking a SARS-CoV-2 outbreak in a Minnesota school system. Understanding how and where the coronavirus was spreading helped local officials implement restrictions to help keep the public safe. This episode demonstrates how clinical laboratories that can quickly sequence SARS-CoV-2 accurately and at a reasonable cost will give public health officials new tools to manage the COVID-19 pandemic.
Officials in Carver County, Minn., used the power of genomic epidemiology to map the COVID-19 outbreak, and, according to the Star Tribune, revealed how the B.1.1.7 variant of the SARS-CoV-2 coronavirus was spreading through their community.
“The resulting investigation of the Carver County outbreak produced one of the most detailed maps of COVID-19 transmission in the yearlong history of the pandemic—a chart that looks like a fireworks grand finale with infections producing cascading clusters of more infections,” the Star Tribune reported.
Using genetic sequencing, the Minnesota Department of Health produced the above map of the spread of the COVID-19 through Carver County’s schools. The animated graph includes epidemiological data from “10 high school teams, 10 club teams, 12 teams in a sports association, and three fitness/rec centers.” According to the Star Tribune, “The cluster shows a high ‘attack rate’ of infected people spreading the virus to multiple close contacts. Genomic sequencing found the more infectious B.1.1.7 variant of the virus in about a quarter of cases so far.” Click here to access the interactive version of the map. To see details about specific persons and locations, tap or hover over each dot. (Graphic copyright: Minnesota Department of Health/Star Tribune.)
Private Labs, Academic Labs, Public Health Labs Must Work Together
For gene sequencing to guide policy and decision making as well as it did in Carver County, coordination, cooperation, and standardization among public, private, and academic medical laboratories is required. Additionally, each institution must report the same information in similar formats for it to be the most useful.
“Maintain Policies That Slow Transmission: Variants will continue to emerge as the pandemic unfolds, but the best chance of minimizing their frequency and impact will be to continue public health measures that reduce transmission. This includes mask mandates, social distancing requirements, and limited gatherings.
“Prioritize Contact Tracing and Case Investigation for Data Collection: Cases of variants of concern should be prioritized for contact tracing and case investigation so that public health officials can observe how the new variant behaves compared to previously circulating versions.
“Develop a Genomic Surveillance Strategy: To guide the public health response, maximize resources, and ensure an equitable distribution of benefits, the US Department of Health and Human Services (HHS) should develop a national strategy for genomic surveillance to implement and direct a robust SARS-CoV-2 genomic surveillance program, drawing on resources and expertise from across the US government.
“Improve Coordination for Genomic Surveillance and Characterization: There are several factors in creating a successful genomic surveillance and characterization network. Clear leadership and coordination will be necessary.”
Practical Application of Genomic Sequencing
Genomic epidemiology uses the genetic sequence of a virus to better understand how and where a given virus is spreading, as well as how it may be mutating. Pathologists understand that this information can be used at multiple levels.
Locally, as was the case in Carver County, Minn., it helps school officials decide whether to halt sports for a time. Nationally, it helps scientists identify “hot spots” and locate mutations of the coronavirus. Using this data, vaccine manufacturers can adjust their vaccines or create boosters as needed.
“This is some of the most amazing epidemiology I’ve ever seen,” epidemiologist Michael Osterholm, PhD, Regents Professor, and Director of the Center for Infectious Disease Research and Policy (CIDRAP) at the University of Minnesota, told the Star Tribune, which reported that “A public health investigation linked 140 COVID-19 cases among more than 50 locations and groups, mostly schools and sports teams in Carver County. (Photo copyright: University of Minnesota.)
Will Cost Decreases Provide Opportunities for Clinical Laboratories?
Every year since genomic sequencing became available the cost has decreased. Experts expect that trend to continue. However, as of now, the cost may still be a barrier to clinical laboratories that lack financial resources.
“Purchasing laboratory equipment, computer resources, and staff training requires significant up-front investments. However, the cost per sequence is far less today than it was under earlier methods,” the GAO noted. This is good news for public and independent clinical laboratories. Like Carver County, a significant SARS-CoV-2 outbreak in the future may be averted thanks to genetic sequencing.
“The first piece of the cluster was spotted in a private K-8 school, which served as an incubator of sorts because its students live in different towns and play on different club teams,” the Star Tribune reported.
Finding such clusters may provide opportunities to halt the outbreak. “We can try to cut it off at the knees or maybe get ahead of it,” epidemiologist Susan Klammer with Minnesota Public Health and for childcare and schools, told the Star Tribune.
This story is a good example of how genomic sequencing and surveillance tracking—along with cooperation between public health agencies and clinical laboratories—are critical elements in slowing and eventually halting the spread of COVID-19.
Though pathology salaries rank 16th among 29 medical specialties, it is in the top 10 among specialties that attract women and respondents say that comes with a lot of paperwork
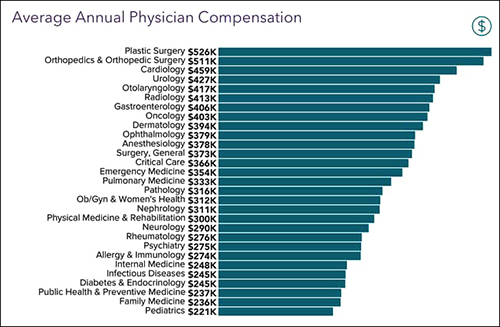
Despite “hardships” brought on by the COVID-19 pandemic, 18,000 physicians in more than 29 medical specialties who participated in Medscape’s 2021 Physician Compensation Report said that, overall, their 2020 income was similar to prior years. Pathologists reported earnings in 2020 of $316,000, $28,000 below the average specialist’s salary of $344,000.
The average pathologist’s salary ranked 16th among medical specialty salaries.
Compared to 2019, medical specialists on average made $2,000 less in 2020. The average salary for primary care doctors was $242,000 in 2020, down $1,000 from 2019, according to a Medscapenews release.
“Physicians experienced a challenging year on numerous fronts, including weathering the volatile financial impact of lockdowns,” said Leslie Kane, Senior Director, Medscape Business of Medicine, in the news release. “Our report shows that many were able to pivot to use telemedicine and focus on tactics that would protect their practices.”
Medscape, a health information provider that is part of the WebMD network, said that in addition to telehealth, doctors turned to MACRA (Medicare Access and CHIP Reauthorization Act of 2015) value-based payment reward programs and other strategies to minimize the effects of office closures last year.
“COVID took a terrible emotional toll on physicians and healthcare workers, and many are still struggling financially, but our findings showed that physicians will innovate and change quickly to meet the needs of patients through extremely difficult times,” said Leslie Kane (above), Senior Director, Medscape’s Business of Medicine, in the news release. Pathologists who were at the center of the nation’s COVID-19 pandemic response would likely echo her sentiments. (Photo copyright: Medscape.)
Pathology Salary Unchanged
To complete its study, Medscape asked physicians to take a 10-minute online survey. The reported findings included responses from 17,903 physicians (61% male, 36% female) practicing in more than 29 specialties between October 2020 and February 2021.
Pathologists who participated in the survey reported no change in their annual salary since 2019. Other specialties that reported no salary change include:
Family medicine,
Infectious diseases,
Ophthalmology, and
Orthopedics/orthopedic surgery.
Top 10 Medical Specialty Salaries
Medscape’s report listed these top-10 medical specialties as earning the highest salaries (see the graphic below for the full list of medical specialties surveyed):
Contrary to what many specialists reported, plastic surgeons did not experience slowdowns in appointments during the COVID-19 pandemic. In fact, not only did plastic surgeons earn the most, at 10% they are the medical specialists who got the biggest increase in pay of previous years as well.
According to the American Academy of Facial Plastic and Reconstructive Surgery (AAFPRS), which conducted its own salary survey of its member surgeons, “70% of AAFPRS surgeons report an increase in bookings and treatments over the course of the COVID-19 pandemic, with nine in 10 facial plastic surgeons indicating an increase of more than 10%. Surgical procedures are the most common procedures as part of this upsurge, perhaps cancelling out any decreases that might have resulted from the economic crisis and lockdowns.”
Other specialist salaries which Medscape found increased in 2020 include:
Oncology: up 7%
Rheumatology and cardiology: up 5%
Diabetes/endocrinology: up 4%
Neurology, critical care, psychiatry: up 3%
General surgery, urology, public health/preventive medicine: up 2%
Medical specialties that reported reductions in salary included:
Otolaryngology and allergy/immunology: down 9%
Pediatrics and anesthesiology: down 5%
Dermatology: down 4%
Pulmonary medicine, physical medicine, gastroenterology, and radiology: down 3%
Emergency medicine and internal medicine: down 1%
About 92% of physicians surveyed indicated that the COVID-19 pandemic caused their income to decline. Also, 22% of doctors noted they experienced loss of work hours.
Pathologists Received Low Average Bonuses
Reporting on receipt of incentive bonuses, Medscape ranked pathology in the bottom half of its list with $42,000 as an average bonus. The top incentive bonuses went to those practicing:
Orthopedics/orthopedics surgery: $116,000
Ophthalmology: $87,000
Otolaryngology: $72,000
About 59% of primary care physicians and 55% of specialists surveyed reported receiving an incentive bonus.
Pathologists Rank High in Job Satisfaction
In responding to a question about compensation, pathologists ranked near the top (seventh position) with 64% saying they are content with their pay. Others expressing salary satisfaction included:
Oncology: 79%
Psychiatry: 69%
Plastic surgery: 68%
Dermatology: 67%
Public health/preventive medicine: 66%
Radiology: 65%
Pathology: 64%
Pathology Popular Among Women MDs
Medscape found that women MDs chose certain medical specialties more often than others, including pathology, which ranked eighth. The top eight specialties employing female physicians are:
Pediatrics: 61%
Obstetrics/gynecology: 59%
Diabetes/endocrinology: 50%
Family medicine: 47%
Dermatology: 46%
Infectious diseases: 46%
Internal medicine: 44%
Pathology: 43%
Specialties with the fewest female physicians are:
Plastic and general surgery: 20%
Cardiology: 14%
Urology: 11%
Orthopedics/orthopedics surgery: 9%
Pathology a Leader in Paperwork
Medscape also surveyed physicians as to the estimated hours they spend per week on paperwork and administration. Here, pathology ranked the fifth highest with 19%, while radiologists and hospital-based physicians were third from the bottom with 11.6%.
Specialists that reported the highest hours spent on paperwork include:
Amid a trying year, the Medscape survey respondents made an encouraging point: 78% of them said they would choose medicine as a career again. And 85% of pathologists said they would choose the same specialty.
Medscape’s report may be helpful to hospital-based clinical laboratory leaders preparing salary budgets and to pathologists in salary negotiations and determining professional responsibilities.
Clinical laboratories may see increase in flu and COVID-19 specimen processing as people return to pre-pandemic social behaviors, experts predict
While SARS-CoV-2 infections continue to ravage many parts of the world, influenza (flu) cases in North America have hit a historic low. As winter approached last year, infectious disease experts warned of a “twindemic” in which the COVID-19 outbreak would combine with seasonal influenza to overwhelm the healthcare system. But this did not happen, and many doctors and medical laboratory scientists are now investigating this unexpected, but welcomed, side-effect of the pandemic.
From the start of the current flu season in September 2020, clinical laboratories in the US reported that 1,766 specimens tested positive for flu out of 931,726—just 0.2%—according to the CDC’s Weekly US Influenza Surveillance Report. That compares with about 250,000 positive specimens out of 1.5 million tested in the 2019-2020 flu season, the CDC reported. Public health laboratories reported 243 positive specimens out of 438,098 tested.
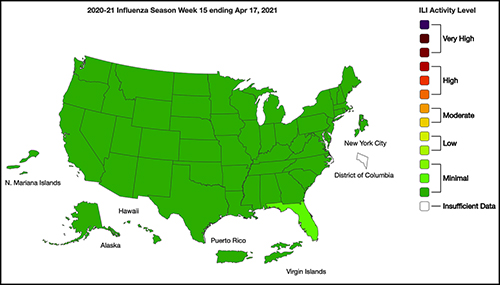
The graphic above taken from the CDC’s Weekly Influenza Surveillance Report for the week ending April 17, 2021, illustrates how “Nationwide during week 15, 1.1% of patient visits reported through ILINet were due to ILI [Influenza-like Illness].” This percentage, according to the CDC, is below the national baseline of 2.6%. “Seasonal influenza activity in the United States remains lower than usual for this time of year.” (Graphic copyright: Federal Centers for Disease Control and Prevention.)
Fear of COVID-19 Linked to Fewer Flu Deaths in Children
WebMD reported that just one child in the US has died from the flu this year, compared with 195 in 2020. Why the low numbers?
Precautions people take to avoid COVID-19 transmission, including masking, social distancing, and handwashing.
Reduced human mobility, including less international travel.
Higher-than-usual flu vaccination rates. As of February 26, the CDC reported that nearly 194 million doses of flu vaccine had been distributed in the US.
WebMD noted this could be a record, but that the CDC data doesn’t indicate how many doses were actually administered.
However, Schaffner told WebMD that efforts to keep kids home from school and away from social gatherings were likely a bigger factor. “Children are the great distributors of the influenza virus in our society,” he said. But due to fears about COVID-19 transmission, kids “weren’t even playing together, because mothers were keeping them off the playground and not having play dates.”
Repercussions for Fighting Flu Next Year
Public health experts welcomed the low flu levels, however, Politico reported that limited data about flu circulation this year could hamper efforts to develop an effective vaccine for next season’s flu strains.
Each February, Politico explained, experts convened by the World Health Organization (WHO) look at data from the current and previous flu seasons to predict which strains are likely to predominate in the Northern Hemisphere next winter. That includes data about which strains are currently circulating in the Southern Hemisphere. The WHO uses these predictions to recommend the composition of flu vaccines. In the US, the final decision is made by an FDA advisory committee.
A similar WHO meeting in September guides vaccine development in the Southern Hemisphere.
The WHO issued this year’s Northern Hemisphere recommendations on Feb. 26. The advisory includes recommendations for egg-based and cell- or recombinant-based vaccines, and for quadrivalent (four-strain) or trivalent (three-strain) vaccines.
In a document accompanying the recommendations, the WHO acknowledged concerns about this year’s limited pool of data.
“The volume of data available from recently circulating influenza viruses, and the geographic representation, have been significantly lower for this northern hemisphere vaccine recommendation meeting than is typical,” the document stated. “The reduced number of viruses available for characterization raises uncertainties regarding the full extent of the genetic and antigenic diversity of circulating influenza viruses and those likely to pose a threat in forthcoming seasons.”
The report notes that experts identified changes in circulating Influenza A(H3N2) viruses this year, and that the changes are reflected in the new vaccine recommendation.
But Paul A. Offit, MD, who serves on the FDA’s vaccine advisory panel, downplayed worries about the vaccine. “The belief is that there was enough circulating virus to be able to pick what is likely to be the strains that are associated with next year’s flu outbreak,” he told Politico. Offit is a Professor of Vaccinology and Pediatrics at the Perelman School of Medicine at the University of Pennsylvania and Director of the Vaccine Education Center at the Children’s Hospital of Philadelphia.
Pediatrician and internationally recognized expert in the fields of virology and immunology, Paul A. Offit, MD (above), told Politico that the low level of flu circulation this year, along with the resulting uncertainty, “is unprecedented.” Clinical laboratories might not have noticed the severe decrease in influenza specimens sent for processing due to being hyper-focused on COVID-19 testing. But as the pandemic subsides, loss of flu testing revenues will likely become more apparent. (Photo copyright: University of Pennsylvania.)
Offit suggests that efforts to mitigate the COVID-19 outbreak could be useful to combat other infectious disease outbreaks. However, both Offit and Gostin expressed doubt about that prospect.
“I mean, could we reasonably in a winter month, wear masks just at least when we’re outside in large crowds? … Or are we comfortable having hundreds of 1000s of cases of hospitalizations for flu and 10s of 1000s [of] deaths? I suspect the answer is B. We’re comfortable with that, we’re willing to have that even though we just learned, there’s a way to prevent it,” Offit told Politico.
“Remember after the 1918 flu pandemic, most people don’t realize what happened when that was over. But what happened was the roaring ‘20s,” Gostin told Politico. “People started congregating, mingling, hugging, kissing. All the things they missed. They crowded into theaters and stadiums and went back to church. That’s what’s likely to happen this fall and that makes the influenza virus very happy.”
So, what should clinical laboratories expect in future flu and COVID-19 vaccines? That is not yet clear. One thing is certain, though. New lab test panels that test for influenza and the SARS-CoV-2 coronavirus will be arriving in the marketplace.
‘Care Studio’ is designed to give physicians a ‘single, centralized view’ of patients’ records that are spread among multiple disparate databases within a healthcare system
Lack of interoperability between electronic health records (EHRs) has been a thorn in the side of healthcare providers—including clinical laboratorians and pathologists—who have to search multiple healthcare organizations’ databases to pull together medical records on individual patients. Google Health claims it may have the answer to the longstanding issue of siloed patient records.
Google Health and St. Louis-based Ascension, one of the largest healthcare systems in the US, have announced the clinical pilot of their new Care Studio platform. The software tool, according to the Care Studio website, “leverages Google’s expertise in organizing information to help clinicians find health record information faster.
“The tool’s Clinical Search feature,” Google Health continues, “enables nurses and doctors to simply type what they’re looking for and quickly find the specific information requested—which might otherwise require significant time and effort to uncover.”
Essentially, Care Studio complements existing EHR systems and enables healthcare providers to quickly search and organize previously siloed patient healthcare data stored on multiple EHRs within a health system. If successful, such a tool would clearly help streamline physicians’ workflows and shave hours off their daily patient research.
According to Google Health, Care Studio is a cross-platform EHR tool that gives clinicians a “single, centralized view that brings forward a patient’s hospital visits, outpatient events, laboratory tests, medications and treatments, and progress notes.”
Gathered data then can be visualized in tables, graphs, and other formats.
“Using Google’s expertise in organizing complex information, Care Studio (above) provides a unified view of patient records, making them more accessible and useful for clinicians,” Peter Clardy, MD, Senior Clinical Specialist at Google Health, said in the launch video. “In Care Studio, you can browse and search through patient information.” Clinical laboratory test results will be included in these screen views. (Photo copyright: YouTube/Ascension.)
According to Medical Device Network, Google and Ascension originally introduced Care Studio to a small number of providers at Ascension’s Nashville and Jacksonville, Fla., locations. They are now expanding the pilot to more nurses and physicians working in clinical settings.
“So, why Google?” David Feinberg, MD (above), VP, Google Health, asked in a video announcement. “Google is really, really good at organizing information, and these electronic health records have amazing amounts of information. But they are unusable. So, we want to bring the functionality of Google—the way to kind of organize information—so doctors can spend more time holding your hand, looking into your eye, and having the difficult conversations with you instead of being data clerks. Part of that is allowing them to find the needle in the haystack in your medical record in seconds, instead of days.” This, of course, would include clinical laboratory test results, which make up 80% of all medical records. (Photo copyright: YouTube/Google Health.)
In a blog post, Eduardo Conrado, Executive Vice President, Strategy and Innovation at Ascension, wrote, “In current EHR systems, clinical information too often is buried in siloed records scattered across hospitals, clinics, urgent care centers, pharmacies, physician offices, labs, and other sites of care, making it challenging for physicians and caregivers to efficiently deliver coordinated and precise care.
“When information is finally retrieved from these disparate EHR systems,” he added, “it is usually poorly organized and fragmented. Most clinicians work in an environment where data is incomplete, inaccessible, and delivered in disjointed bursts of information without context.”
COVID-19 Accelerates Need for Improvements in Data Access
Conrado notes that the ability for clinicians to quickly retrieve and organize a patient’s complete clinical history is “the essence of delivering effective and efficient care.” He wrote that the “once-in-a-generation” COVID-19 pandemic has accelerated the need for improvements in public health infrastructure, health technology services, and care delivery models and “reinforced the significant impact that complex and often confusing EHR systems, and the fragmentation of patient health data, have on delivering effective care.”
While the collaboration between Ascension and Google began in 2018, Conrado said “remarkable” progress was made on Care Studio this past year.
Conrado did not state how long the clinical pilot of Care Studio would last but emphasized that the technology will be enhanced with additional features and improvements based on feedback from pilot clinicians. Ultimately, the clinical search tool will be made available to all caregivers across Ascension’s 2,600 sites of care, including 145 hospitals and more than 40 senior living facilities in 19 states and the District of Columbia.
Clinical laboratories should welcome this development. Any software tool or information technology that allows clinical laboratory test data to move across different EHRs will help interoperability.
Since the early 1980s, UBC’s CMPT program, led by medical microbiologist Michael Noble, MD, has provided external quality assessment (EQA) for clinical microbiology and water testing laboratories. This includes providing biological samples related to:
“Typical of every jurisdiction in North America and probably around the world, BCCDC got swamped beyond swamped,” said Noble, the Clinical Microbiology Proficiency Testing (CMPT) program’s first and current Chair, in an exclusive interview with Dark Daily. “The increase was 10-fold, and they were unable to provide all the services they wanted to do. And since I was already running a proficiency testing program across the province, they asked if I would provide that service for COVID-19 for laboratories that were doing the testing.”
Michael Noble, MD (above), is Professor Emeritus (active) in UBC’s Department of Pathology and Laboratory Medicine and Chair of the Program Office for Laboratory Quality Management (POLQM). He began his career as a medical microbiologist but soon focused on laboratory quality management. Within the Department of Pathology and Laboratory Medicine, Noble co-developed the Clinical Microbiology Proficiency Testing (CMPT) program in 1983, a program he still chairs but will soon pass on to a new leader. (Photo copyright: University of British Columbia.)
CMPT’s Proficiency Testing Serves Labs Worldwide
UBC’s CMPT external quality assessment (EQA) program serves all medical laboratories in British Columbia, as well as other labs in Canada, Europe, South America, and the Caribbean. Just over 200 laboratories currently participate in the program. More labs participated in past years, before lab consolidation affected CMPT and other programs as well, Noble said.
CMPT’s proficiency testing ensures that participant laboratories that have been provided with simulated samples can perform tests at the “level of quality and competence required,” notes UBC’s CMPT website.
“Samples are complex, highly realistic, and clinically relevant. CMPT samples contain host elements as well as targeted pathogens,” Noble explained on his blog, “Making Medical Laboratory Quality Relevant.”
COVID-19 Brings Non-Traditional ‘Laboratories’ to CMPT’s Proficiency Testing Program
UBC’s proficiency testing for SARS-CoV-2, the coronavirus that causes the COVID-19 infection, differs from other CMPT programs. That’s due to new participants that entered the laboratory testing program during the COVID-19 pandemic that are performing COVID-19 testing in non-traditional locations, Noble stated.
“In our proficiency programs, we had mainly been dealing with traditional clinical laboratories,” Noble explained. “But now, we find people doing COVID-19 testing—even though defined as medical laboratories—who are working in airports, or in tourism, or the movie industry, or forestry. They may never have worked in an actual clinical laboratory. So, it’s a very different style of proficiency testing. There has been a lot of handholding, teleconferences, discussions, and one-on-ones with that group,” Noble said.
Participant laboratories receive viral material that “simulates typical samples.” They need to demonstrate proficiency by performing the test and reporting it as positive, negative, or inconclusive.
“Our product is derived from a pure culture of a single strain of SARS-CoV-2, and it appears to be effective for all targets,” Noble stated.
Detecting COVID-19 by Gargling and Rinsing
UBC’s program typically offers simulated sampling for detection of SARS-CoV-2 in nasopharyngeal swabs. However, the BC Center for Disease Control’s (BCCDC) mouth rinse and gargle sample collection for diagnosis of COVID-19 also is available and widely used in Canada, Noble said.
In his career, Noble transitioned from medical microbiology to qualitology, which he describes as “the study of quality in the medical laboratory.”
In stressing the importance of laboratory quality testing, Noble describes the possibility of laboratory testing going awry and leading to a microbiological public health emergency.
“What happens if there’s a stool sample, and someone misses the presence of Campylobacteriosis in the stool? What happens if that’s part of a foodborne disease and there’s an outbreak in the city and samples are being missed? How many people will be impacted as a result of that error?” he asked.
University of British Columbia Endows a Chair for Laboratory Quality Management
Noble says UBC’s Program Office for Laboratory Quality Management (POLQM) has involved organizations worldwide and certified more than 500 people.
“The impact they have over their laboratories has been huge. Maybe that would have happened without us. But we were a part of that. And our impact is not one laboratory or one city or one province but widespread, and that’s a real and enriching experience to have,” he said.
But now it is time for him to move on. Noble secured (through UBC), a benefactor to establish the endowed Chair for Laboratory Quality Management. The family of the late Donald B. Rix, MD, a Canadian pathologist and philanthropist, gave $1.5 million (matched by the university) to create the Associate Professor (Grant Tenure) Donald B. Rix Professorship in Laboratory Quality at UBC, Department of Pathology and Laboratory Medicine.
Long-serving pathologists and medical laboratory professionals may remember that Rix was the founder and chair of MDS Metro Laboratory Services (now known as LifeLabs Medical Laboratory Services). It grew into the largest private medical laboratory in Western Canada.
Referring to this endowed new Chair for Laboratory Quality Management, Noble said, “I think this is the first named position of laboratory quality in North America.” UBC has commenced reviewing applications for the position, which is expected to be effective in January 2022. Pathologists and clinical laboratory scientists with appropriate qualifications and interest in this position should contact Dr. Noble’s office at the University of British Columbia Faculty of Medicine.