Government prosecutors allege destruction of LIS database and point to Holmes’ extravagant lifestyle as evidence of fraud motive
There is a new twist in the federal criminal fraud trial of Elizabeth Holmes, co-founder and former CEO of now defunct clinical laboratory testing company Theranos. Once again, the trial has been delayed. In the meantime, however, dueling court filings between prosecutors and defense lawyers have shed additional light on the allegations against Holmes and co-defendant Ramesh Balwani, the company’s chief operating officer. The revelations will be of interest to medical laboratory leaders.
According to The Mercury News, United States District Judge Edward J. Davila cited the ongoing COVID-19 pandemic in his December 18 ruling that postponed the start of Holmes’ trial to July 13, 2021.
In his ruling, Judge Davila wrote, “The court notes sadly, the impact on our lives is grim. California is in the midst of an unprecedented surge in cases and hospitalizations.”
The judge also noted the prospects for widespread public vaccination in the coming months. “All of this supports continuing the trial [of Holmes] to a time when our community is safer,” he added. “The court recognizes that a continuance of the trial will cause great inconvenience to victims who would like their day in court, as well as Defendant, who wishes a speedy opportunity to defend against the charges. All of these rights are important, but paramount to the court is the safety and health of the community.”
On February 9, Law360 reported that Balwani’s trial was delayed even further, with jury selection now set to begin on January 11, 2022.
Wall Street Journal Exposé of Theranos and its Flawed Clinical Lab Testing
In “Elizabeth Holmes: The Breakthrough of Instant Diagnosis,” the Wall Street Journal (WSJ) put Holmes squarely in the public eye. It could be credibly asserted that the paper’s fawning coverage helped boost her credibility when no one knew who she was. Thus, it is ironic that just two years later it was the WSJ that, in a series of articles, exposed the alleged misrepresentation and fraud committed by Holmes, Balwani, and Theranos.
By 2015, the company had a stock valuation of $9 billion, but it all came crashing down after WSJ investigative journalist John Carreyrou revealed serious problems with the company’s management and technology.
In a public notification from the US Attorney’s Office Northern District of California, the government alleged that Holmes and former Theranos president Balwani promoted the company’s blood-testing technology despite knowing that it was likely to produce unreliable results.
The defendants now face 12 federal felony counts related to wire fraud. They have pleaded not guilty. According to The Mercury News, if found guilty of all charges, “Holmes faces a potential 20-year prison sentence, up to $2.75 million in fines, and possible restitution to investors the government alleges lost more than $700 million.”
Elizabeth Holmes (above), former CEO of now defunct clinical laboratory testing company Theranos, will now stand trial starting in July. Due to risk of infection from the SARS-CoV-2 coronavirus, jurors will be required to wear masks and to socially distance during the trial, CNBC reported. What will be of great interest to clinical laboratories are statements by federal prosecutors that testing data stored on the company’s laboratory information system was destroyed before it could be accessed by investigators, even though it had been subpoenaed months earlier by a federal grand jury. (Photo copyright: Forbes/Yichuan Cao/NurPhoto via Getty Images.)
Missing Clinical Laboratory Data
Though the trial has been delayed, attorneys on both sides have been busy. Last November, after failing to have the charges dismissed, defense attorneys filed a flurry of motions seeking to exclude much of the government’s evidence, The Mercury News reported. This included expert witnesses, testimony about inaccurate test results, and numerous news articles about the company and its tests.
Prosecutors responded to the motions in January, further illuminating their case while providing more fodder for media coverage.
In a January 11 filing [doc-682], the government alleged that a Theranos laboratory information system (LIS) containing patient test results and quality control data was destroyed “on or about August 31, 2018—three months after a federal grand jury issued a subpoena requesting a working copy of this database.” News of the allegation was first reported by The Register, a UK-based IT publication.
Previously, the prosecutors alleged, Theranos, with assistance from an IT contractor, had provided a backup copy of the database to the government but without a password needed for decryption. “All subsequent efforts by the government to access the data on this hard drive have failed,” even with assistance from a computer forensics expert, they wrote.
Then, the original database was permanently destroyed in August when Theranos moved out of its facility in Newark, Calif., the government alleged in its filing. “On or about August 31, 2018—three months after a federal grand jury issued a subpoena requesting a working copy of this database—the LIS was destroyed. The government has never been provided with the complete records contained in the LIS, nor been given the tools, which were available within the database, to search for such critical evidence as all Theranos blood tests with validation errors,” the filing read.
The January 11 filing was in response to a Theranos motion [doc-563] seeking to exclude evidence of “anecdotal test results.”
“The data disappeared. Defendant should be barred from arguing the government’s case is anecdotal when Theranos (and others) destroyed this data,” the prosecutors argued.
Furthermore, prosecutors wrote, “the government’s case is hardly ‘anecdotal.’ The reliability and accuracy problems in Theranos’ clinical lab were well-documented when the Centers for Medicare and Medicaid Services (CMS) investigated the lab, discovered the accuracy and reliability problems, and determined Theranos could not safely administer its tests on patients. Whistleblowers will also testify about Theranos’ accuracy and reliability problems. And patients themselves experienced these problems, receiving incorrect results that affected their treatment and deprived them of the benefit of the purportedly reliable blood tests for which they had paid.”
And Then There’s Her Lifestyle
Prosecutors also claimed in their filing that Holmes’ activities—which included “travel on private jets, stays in luxury hotels, and access to multiple assistants … [who] handled a range of non-business tasks for Defendant, including personal clothes and jewelry shopping, home decorating, food and grocery buying, and other items”—shows that Holmes was “funding an extravagant lifestyle … through company money,” CNBC reported.
And so, the saga of Theranos continues. Will Elizabeth Holmes succeed in her defense? Could a clinical laboratory phoenix bird rise from the ashes of this failed lab test company? Who knows? Probably not. But until there is a resolution, we will keep reporting on the case.
Called the Geographic Direct Contracting Model (GEO), CMS’ new “voluntary payment model” aims at giving providers of Medicare Part A and Part B services “a direct incentive to improve care across entire geographic regions,” according to a CMS press release.
“The Geographic Direct Contracting Model is part of the Innovation Center’s suite of Direct Contracting models and is one of the Center’s largest bets to date on value-based care,” Brad Smith, Deputy Administrator and Director of the Center for Medicare and Medicaid Innovation (CMMI), told RevCycleIntelligence. Smith is also the former CEO and co-founder of Aspire Health.
According to a CMS Fact Sheet, the GEO model “will test whether a geographic-based approach to value-based care can improve quality of care and reduce costs for Medicare beneficiaries across an entire geographic region.”
“This model allows participating entities to build integrated relationships with healthcare providers and invest in population health in a region to better coordinate care, improve quality, and lower the cost of care for Medicare beneficiaries in a community, said CMS Administrator Seema Verma in the CMS press release. Clinical laboratories may find opportunities as well, to collaborate with physicians in the clinical decision-making process. (Photo copyright: Business Insider.)
“Leveraging best practices and lessons learned from prior Innovation Center models, Geo will enable Direct Contracting Entities (DCEs) to build integrated relationships with healthcare providers and community organizations in a region to better coordinate care and address the clinical and social needs of Medicare beneficiaries,” the CMS Fact Sheet states.
“If we’re successful, we’ll move value-based care from something that might be 10 or 20% of somebody’s revenue to something that’s 80 or hopefully 100% of somebody’s revenue (in five to 10 years),” Smith told MedPage Today.
Healthcare providers and health plans that participate in the Geographic Direct Contracting model must be covered entities under the Health Insurance and Portability Accountability Act (HIPAA) and submit applications by April 2, 2021, the CMS fact sheet states.
The first performance period starts Jan. 1, 2022, and participation is voluntary. Direct contracting entities take “100% shared savings and shared losses for Medicare Part A and B services for aligned Medicare fee for service beneficiaries in a defined region,” the CMS fact sheet explained.
CMS is considering implementing the GEO model in Atlanta, Dallas, Denver, Detroit, Houston, Los Angeles, Miami, Minneapolis, Orlando, Phoenix, Philadelphia, Pittsburgh, Riverside, San Diego, and Tampa.
“By initially testing the model in a small number of geographies, we will be able to thoughtfully learn how these flexibilities are able to impact quality and costs,” Smith told RevCycleIntelligence.
How Will Value-Based Care Programs Affect Clinical Laboratories?
Value-based payment arrangements require doctors to accept changes to how they are reimbursed for their services. In kind, doctors are examining how clinical laboratories can take on an enhanced role in clinical decision making.
“Physicians and hospitals in a value-based environment need a different level of service and professional consultation from the lab and pathology group because they are being incented to detect disease earlier and be active in managing patients with chronic conditions to keep them healthy and out of the hospital,” said Robert Michel, Publisher and Editor-in-Chief of Dark Daily and its sister publication The Dark Report.
Michel explained that value-based care providers are calling on labs to go beyond reporting accurate test results within allotted turnaround times. “They want collaboration in identifying at-risk patients and in finding and closing gaps in care by using laboratory test results.”
Medical laboratory leaders may want to reach out to healthcare providers participating in value-based care models to explore areas of interest relating to patient population, chronic conditions, and severity of illness.
Clinical laboratories that offer testing and reporting and additionally collaborate with healthcare providers and health plans in ways that contribute to improved patient outcomes and lowered costs, may be in a position to earn any financial rewards from these and other new value-based arrangements.
Available funds and disease prevalence affect whether pooled testing is feasible and desirable, notes University of Kansas Health System microbiology laboratory director
Pooled testing for the SARS-CoV-2 coronavirus has its supporters and its critics. There is no one-size-fits-all when it comes to pooling multiple patients’ biological samples into a single COVID-19 test in the hopes that the result will be all negative. Several factors must be in place for COVID-19 pooled testing to be viable at individual clinical laboratories. The experience of medical labs that considered doing pooled testing are informative.
For example, when Rachael Liesman, PhD, Director of Microbiology in Pathology and Laboratory Medicine at the University of Kansas Health System in Kansas City, researched developing a plan for pooled testing of COVID-19 patients for her health system, she found the strategy less than ideal for two reasons:
First was the rate of infection in the population being tested. If the rate was too high, pooled testing produced too many positive results, making the process impractical.
Second was the need for expensive automated equipment in the microbiology laboratory, the funding to buy that equipment, and the room to accommodate it.
Last summer, as Liesman and her microbiology lab staff were evaluating pooled testing, she spoke with Dark Daily’s sister publication The Dark Report. “We were trying to decide whether pooled testing really would save us anything,” she said in the exclusive interview. “We were looking at the barriers and trying to understand what we’d gain and what we’d lose.”
Deciding Against Pooled Testing at University of Kansas Health System
After careful consideration, the lab staff stopped considering pooled testing due to increased prevalence in the community, Liesman said in December. “Our positivity rate is double what we were seeing in the summer,” she noted.
“Of course, the biggest challenge with pooling specimens is you have to have a patient population that has a low enough virus prevalence to make it worth your time,” she noted. “For us, there may be some patient populations that have a low enough level of prevalence, but not enough to make pooling feasible.”
University of Kansas Health System’s microbiology laboratory has been running 800 to 1,000 COVID-19 molecular tests 24 hours a day, seven days a week, although the lab runs fewer tests on the weekends. On Jan. 8, the number of new coronavirus cases in Kansas was at 1,780 per million, according to the COVID Tracking Project (CTP). That was about the highest rate since the pandemic began early in the year.
“Pooling makes a lot of sense for massive high-volume reference labs. I don’t have the capacity to run 6,000 specimens a day through my lab,” noted Rachael Liesman, PhD (above), Director of Microbiology in Pathology and Laboratory Medicine at the University of Kansas Health System, in an exclusive interview with The Dark Report. Not all clinical laboratories can or should consider pooled testing, which Dark Daily noted in previous e-briefings. (Photo copyright: Twitter.)
“One of the challenges in any lab is when you get specimens arriving in volume of say 100 or 200 specimens every few hours,” Liesman explained. “When that happens, you have to determine rapidly which of those specimens you would want to pool and which of them you wouldn’t pool. Or, if you had the right circumstances, you could pool all of them.
“You might have asymptomatic patients in one group and symptomatic patients in another group. So, then you could put all samples from one group into a pool. But if you’re not set up that way, just figuring that part out could be really time consuming,” she noted.
“Another challenge,” Liesman added, “is if your laboratory doesn’t have liquid handlers, which are the instruments that do the pooling for you.”
Manual versus Automated Pooling
In a clinical laboratory without liquid handlers, the task of pooling is not automated and instead requires staff to do the work manually—one specimen and one pool at a time.
Without the right equipment, Liesman noted, somebody in the lab must physically take five tubes and combine them in into one tube. And that one person has to ensure the test tube of pooled specimens is appropriately stickered. Then, once that is completed, the information must be input into the laboratory information system (LIS).
“We have a liquid handler because we purchased one from Hamilton specifically for COVID testing. But getting all that information into the computer system can take a lot of time,” she said. “A lot of labs don’t have access to this type of instrumentation, which means the process becomes very hands-on.
“We already see repetitive-use injuries, and if many of your staff are spending their eight-hour shifts doing pipetting motions, then they’re at greater risk for repetitive-use injury,” she added.
In addition, having humans doing repetitive motions in a clinical laboratory increases the risk of specimen-handling errors such as tubes being mislabeled or misplaced. “Those mistakes are very hard to find,” Liesman noted. “For us, we’ve been asking if we have the resources to do pooling successfully. And, if we put all these resources into it, what do we gain? That’s the big question for us.”
For a clinical laboratory to successfully initiate and maintain an effective program for pooled testing of the SARS-CoV-2 coronavirus, it must have specific equipment available to reduce manual touches of the specimens and automate as many work processes as possible. The lab’s manager must also consider the staffing required to handle pooled testing. Even then, if disease prevalence climbs above a certain level, pooled testing will not be a viable solution.
These are the reasons why many medical laboratories have considered a pooled testing arrangement but decided it would not be appropriate for their organization. Meanwhile, at other clinical labs pooled SARS-CoV-2 testing has been a major success, partly because it enables the labs to test many more patients using the same quantity of test kits and related supplies.
The No Surprises Act, passed as part of the COVID-19 relief package, ensures patients do not receive surprise bills after out-of-network care, including hospital-based physicians such as pathologists
Consumer demand for price transparency in healthcare has been gaining support in Congress after several high-profile cases involving surprise medical billing received widespread reporting. Dark Daily covered many of these cases over the years.
Now, after initial opposition and months of legislative wrangling, organizations representing medical laboratories and clinical pathologists have expressed support for new federal legislation that aims to protect patients from surprise medical bills, including for clinical pathology and anatomic pathology services.
The new law Congress passed is known as the No Surprises Act (H.R.3630) and is part of the $900 billion COVID relief and government funding package signed by President Trump on December 27.
The law addresses the practice of “balance billing,” in which patients receive surprise bills for out-of-network medical services even when they use in-network providers. An ASCP policy statement noted that “a patient (consumer) may receive a bill for an episode of care or service they believed to be in-network and therefore covered by their insurance, but was in fact out-of-network.” This, according to the ASCP, “occurs most often in emergency situations, but specialties like pathology, radiology, and anesthesiology are affected as well.”
Most portions of the No Surprises Act take effect on January 1, 2022. The law prohibits balance billing for emergency care, air ambulance transport, or, in most cases, non-emergency care from in-network providers. Instead, if a patient unknowingly receives services from an out-of-network provider, they are liable only for co-pays and deductibles they would have paid for in-network care.
New Law Bars Pathologists from Balance Billing without Advance Patient Consent
The law permits balance billing under some circumstances, but only if the patient gives advance consent. And some specialties, including pathologists, are barred entirely from balance billing.
The law also establishes a process for determining how healthcare providers are reimbursed when a patient receives out-of-network care. The specifics of that process proved to be a major sticking point for providers. In states that have their own surprise-billing protections, payment will generally be determined by state law. Otherwise, payers and providers have 30 days to negotiate payment. If they can’t agree, payment is determined by an arbiter as part of an independent dispute resolution (IDR) process.
Early Proposal Drew Opposition
An early proposal to prohibit surprise billing drew opposition from a wide range of medical societies, including the ASCP, CAP, and the American Medical Association (AMA).
All were signatories to a July 29, 2020, letter sent to leaders of the US Senate and House of Representatives urging them to hold off from enacting surprise billing protections as part of COVID relief legislation. Though the groups agreed in principle with the need to protect patients from surprise billing, they contended that the proposed legislation leaned too heavily in favor of insurers, an ASCP news release noted.
“Legislative proposals that would dictate a set payment rate for unanticipated out-of-network care are neither market-based nor equitable, and do not account for the myriad inputs that factor into payment negotiations between insurers and providers,” the letter stated. “These proposals will only incentivize insurers to further narrow their provider networks and would also result in a massive financial windfall for insurers. As such, we oppose the setting of a payment rate in statute and are particularly concerned by proposals that would undermine hospitals and front-line caregivers during the COVID-19 pandemic.”
On December 11, leaders of key House and Senate committees announced agreement on a bipartisan draft of the bill that appeared to address these concerns, including establishment of the arbitration process for resolving payment disputes.
However, in a letter sent to the committee chairs and ranking members, the AHA asked for changes in the dispute-resolution provisions, including a prohibition on considering Medicare or Medicaid rates during arbitration. “We are concerned that the IDR process may be skewed if the arbiter is able to consider public payer reimbursement rates, which are well known to be below the cost of providing care,” the association stated. However, legislators agreed to the change after last-minute negotiations.
“The AHA is pleased that Congress rejected approaches that would impose arbitrary rates on providers, which could have significant consequences far beyond the scope of surprise medical bills and impact access to hospital care,” AHA President and CEO Rick Pollack (above) said in a statement. “We also applaud Congress for rejecting attempts to base rates on public payers.” (Photo copyright: American Hospital Association.)
Dispute Resolution for Pathologists
The CAP also expressed support for the final bill. In a statement, CAP noted that “As the legislation evolved during the 116th Congress, CAP members met with their federal lawmakers to discuss the CAP’s policy priorities.
“Through the CAP’s engagement and collaboration with other physician associations, the legislation improved drastically,” the CAP stated. “Specifically, the CAP lobbied Congress to hold patients harmless, establish a fair reimbursement formula for services provided, deny insurers the ability to dictate payment, create an independent dispute resolution (IDR) process that pathologists can participate in, and require network adequacy standards for health insurers.”
As laboratory testing was identified by thousands of respondents to the University of Chicago survey as the top surprise bill, it is likely that billing and transparency in charges for clinical pathologist and anatomic pathologist will continue to be scrutinized by law makers and healthcare associations.
The remarkably low number of influenza diagnoses makes it possible for clinical laboratories to stay focused on COVID-19
One positive note for clinical laboratories this winter is the fact that the number of biological samples being submitted for influenza (flu) testing have dropped significantly. This has given medical laboratories more resources for processing COVID-19 tests.
According to a feature published in Nature, the number of samples being submitted to medical laboratories for flu testing has dropped by 61%. More surprisingly, the number of positives has dropped by 98%. The combined flu/COVID-19 “twindemic” that some medical experts feared could crush our healthcare system has not materialized—yet, the Washington Examiner reported.
“In any given winter, hospitals are taxed by the flu,” Brian Garibaldi, MD, a pulmonologist and critical care specialist and Medical Director of the Johns Hopkins Biocontainment Unit told the Washington Examiner. “There’s always a concern that our emergency departments will be overwhelmed, and ICU capacity will be strained [due to the concurrence of flu and COVID-19 outbreaks], particularly with people who have coexisting conditions that then get influenza.”
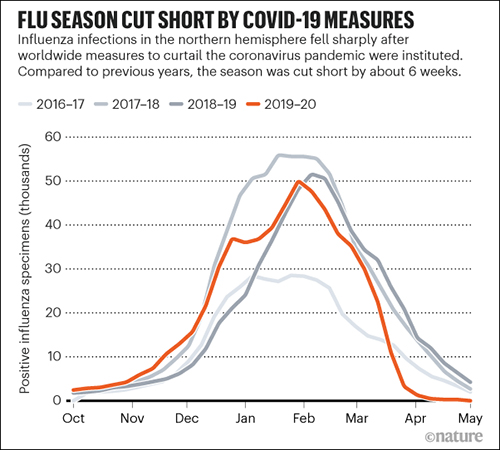
The 2019-2020 flu season ended earlier than usual, likely because of precautions put in place in the spring to combat the coronavirus pandemic. Most years, the seasonal flu in the US peaks in February and trails off by May, Nature reported in “How Coronavirus Lockdowns Stopped Flu in Its Tracks.”
“Seasonal flu cases in the northern hemisphere usually peak in February and tail off by the end of May,” Nature wrote. “This year, unusually, lab-confirmed cases of influenza dropped precipitously in early April, a few weeks after the coronavirus pandemic was declared on 11 March. The data comes from tests of more than 150,000 samples from national influenza laboratories in 71 countries that report data to FluNet, a global surveillance system.”
Government Leaders and Health Experts Remain Concerned
Despite that encouraging data point, public health experts and political leaders were still concerned. In September, Arizona Governor Doug Ducey said, “The overlap of COVID-19 and flu season presents a perfect storm, and we aren’t taking any chances. We are approaching this fall with a proactive mindset and plan of action to limit the impact of the flu and preserve hospital resources,” the Washington Examiner reported.
The caution was certainly warranted. A normal flu season strains resources, but a severe flu season coupled with a global pandemic could have been disastrous. Luckily, Ducey’s “perfect storm” did not materialize.
Data from the World Health Organization’s FluNet Global Influenza Surveillance and Response System was used by Nature to develop the graphic above. It illustrates how the number of positive Influenza specimens in 2019-2020 declined compared to the previous two years. Some experts believe this is due to protocols implemented to combat the COVID-19 coronavirus by hospitals and clinical laboratories. (Graphic copyright: Nature.)
Why Is There Less Influenza?
So, why is there less flu and other respiratory infections?
Epidemiologist Lisa Lockerd Maragakis, MD, MPH, Associate Professor of Medicine and Senior Director of Infection Prevention at Johns Hopkins Health System, told U.S. News, widespread business and school closures provide fewer opportunities for influenza to spread. “We commonly see flu spread in communities, schools, businesses and through travel each year, so those changes are likely keeping the flu away.”
However, this may have a negative effect as well. Eili Klein, PhD, Associate Professor of Emergency Medicine at Johns Hopkins School of Medicine, warns that “Because of the current restrictions and precautions everyone is taking this season, far fewer people will be infected or exposed to the flu virus, and therefore won’t become immune to certain strains of the virus. So, the number of people who may have more severe infections next year is likely to be greater because immunity will be lower,” the Washington Examiner reported.
Other Viral Infections Also in Decline Due to COVID-19 Precautions, Vaccines
Masking, frequent handwashing, and social distancing certainly played a role in reducing the number of cases of flu reported this year. But influenza is not the only disease that saw reductions. “In Hong Kong, compared with previous years, the number of chickenpox cases dropped by about half to three-quarters,” Nature reported. “In April, cases of measles and rubella were their lowest, globally, since at least 2016, according to data available so far.”
Early in the COVID-19 pandemic, some public health officials were concerned that the decline in influenza cases was actually related to a lack of testing. “However, renewed efforts by public health officials and clinicians to test samples for influenza resulted in adequate numbers tested and detection of little to no influenza virus,” the Centers for Disease Control and Prevention (CDC) reported.
Another factor in the lower numbers of flu cases could be due to the fact that more people have gotten vaccinated this year. More than 188 million flu vaccines were distributed in 2020, an increase compared to the 169 million given in 2019.
“Flu vaccination in the community started earlier this year, as recommended by the CDC, and our community physicians report that vaccine uptake has been higher than usual,” Marie-LouiseLandry, MD, Clinical Virologist, Professor of Laboratory Medicine and of Medicine (Infectious Diseases), and Director of the Clinical Virology Laboratory at Yale School of Medicine, told Healthline.
It may also be that influenza diagnoses are fewer because people are not seeking treatment. Hospitals at or beyond capacity due to the pandemic, or fear of contracting COVID-19, may have motivated people with flu-like symptoms to stay home rather than seek treatment. However, most healthcare experts agree that public health measures to fight COVID-19 are likely the larger reason there is less flu.
“Public health measures such as movement restrictions, social distancing, and increased personal hygiene likely had an effect on decreasing influenza and other respiratory virus transmissions,” the World Health Organization (WHO) told Nature.
What About the Next Flu Season?
Experts are more conflicted regarding what all of this means for coming flu seasons. Some experts think that because there’s less flu this year, there will be less immunity next year, and severe illness will result. Others are more optimistic and hope that some strains of flu will disappear, which could mean less flu in the immediate future. It’s not a simple prediction to make.
Even if the low flu numbers this year mean some strains do not survive, it is unlikely that will remain the case. “I am sure that flu will come back with a vengeance at some stage in the future,” Robert Ware, PhD, a biostatistician, clinical epidemiologist, and Professor of Biostatistics with Griffith University in Queensland, Australia, told Nature.
Thus, clinical laboratories should remain vigilant for future influenza outbreaks. Hopefully by then the COVID-19 pandemic will have peaked and labs will be able to reallocate testing resources appropriately.