Consolidation of hospitals and health systems means consolidated medical laboratory services as well, and that impacts laboratory revenue and staff
Though COVID-19 shifted many healthcare systems’ priorities in 2020—including quite dramatically altering the priorities of the nation’s clinical laboratories—the SARS-CoV-2 pandemic does not appear to have slowed the pace of healthcare mergers and acquisitions. Many such deals are kept secret until closed by Dec. 31. They are then then announced after Jan. 1, so we may see additional big and surprising healthcare acquisitions announced in coming weeks.
Leaving aside the shock waves brought about by COVID-19, transformational changes to the healthcare community have been underway for a while.
In his article on HealthManagement.org, healthcare consultant Paul D. Vitale, MPA, FACHE, noted that for the past several years, health systems have set records in the mergers and acquisitions space. In 2017, he noted, there were more than 115 deals, and by 2019, there was a series of “mega” mergers, each worth more than $10 billion. The pattern continued in 2020, even with economic concerns brought about by the pandemic.
“According to many health systems, acquiring another organization, or merging with it, holds the key to future success. Faced with intense pressure to cut back on costs, mergers and acquisitions can leverage the economies of scale,” he wrote.
Below are several “deals” that closed in 2020 or are expected to close in 2021.
Pre-merger, Atrium Health’s network included 41 hospitals and 900 care locations, while the Wake Forest Baptist Health system was comprised of 42 hospitals and 1,500 care locations. Plans are underway to build a second campus for the school of medicine, where 3,500 students will be trained in more than 100 specialized programs.
“The impact of the strategic combination will be far-reaching, elevating North Carolina as a clear destination of choice to receive medical care for people all across the nation,” Julie Ann Freischlag, MD (above), CEO of Wake Forest Baptist Health and Dean of Wake Forest School of Medicine, told Healthcare Finance News. “Through our combined, nationally recognized clinical centers of excellence in multiple specialties, we will be able to expand our research in signature areas, such as cancer, cardiovascular, regenerative medicine and aging, and target bringing research breakthroughs to the community in less than half the time of the national average.” Freischlag will serve as Atrium Health’s Chief Academic Officer as well. (Photo copyright: Triad Business Journal.)
Doctors Acquire a Controlling Stake of Steward Health Care
In June, physicians in Dallas purchased a controlling stake of Steward Health Care through a structured recapitalization transaction. Though not strictly a merger and acquisition, the deal represents a similar transformational change of a health system. The change makes Steward the largest physician-owned-and-operated health system in the country, noted a news release.
Ralph de la Torre, MD (above), CEO and founder of Steward, says the industry is in the midst of a transformational moment. “The COVID-19 global pandemic has exposed serious deficiencies in the world’s healthcare systems, with a disproportionate impact on underserved communities and populations,” he stated in the news release. “We believe that future healthcare management must completely integrate long-term clinical needs with investments. As physicians first, we will focus on creating structures and timelines that meet the long-term clinical needs of our communities and the short-term needs of our patients.” (Photo copyright: The Boston Globe.)
Harrington Healthcare System and UMass Memorial Health Care
In January 2020, Harrington Healthcare of Massachusetts announced it was pursuing a corporate affiliation with UMass Memorial Health Care. The transaction was expected to be finalized by 2021.
“When we entered into our initial agreement with UMass Memorial in January, we had no idea what the next several months would bring,” said Ed Moore (above), President and CEO of Harrington Healthcare, in a news release. “Our team performed exceptionally well, and the community supported us every step of the way, but we could not have provided the outstanding care we did without the partnership and support of the clinical team at UMass Memorial. This experience redoubled our confidence that becoming part of the system would offer maximum benefit to our community at a time that requires flexibility, scale, and resources.” (Photo copyright: Worcester Telegram.)
Will More Announcements Come in 2021? Probably
For clinical laboratory managers and pathologists, the healthcare mergers and acquisitions of greatest interest are those that involve hospitals and health systems. When two big health systems merge—such as the transaction involving Atrium Health and Wake Forest Baptist Health—one of the first clinical services to undergo rationalization and consolidation is the clinical laboratory. One reason for this is because it is much easier to move more lab test specimens around the system than it is to move patients. So, many healthcare merger and acquisition deals directly affect the medical laboratory professionals employed by the institutions involved in the transaction.
Despite the pandemic—or because of the financial stresses created by it—there continue to be strong buyers and financially-weak sellers. For this reason alone, pathologists and clinical laboratory administrators should expect to see a regular flow of merger or acquisition announcements involving major healthcare organizations during 2021.
Developers of medical laboratory tests had high hopes that cheap saliva-based tests would compete with at-home OTC tests that use nasal swabs, but skepticism among scientists continues
Reverse-transcription polymerase chain reaction (RT-PCR) technology has become the standard for clinical laboratory diagnostic testing used to detect the presence of the SARS-CoV-2 coronavirus. However, to enable more widespread testing, some public health experts have called for deployment of cheap, rapid, saliva-based antigen tests that could be self-administered by consumers in their homes.
Despite the technology’s lower sensitivity compared with RT-PCR testing, the idea of “fast-and-frequent” universal antigen testing has gained support as a possible game-changer against the outbreak, the New York Times reported.
The FDA recently took a step in this direction with its first emergency use authorization for the Ellume COVID-19 at-home antigen test. But other developments suggest that these tests may fall short of the lofty vision initially outlined by the experts.
Ellume’s COVID-19 Home Test (above) received emergency use authorization from the FDA on December 15. In a press release, Ellume claimed its rapid-antigen test, “demonstrated a sensitivity of 96% and specificity of 100%, and in asymptomatic individuals, the test demonstrated a sensitivity of 91% and specificity of 96%. This level of accuracy across both symptomatic and asymptomatic individuals is crucial in mitigating the spread of an infectious disease like COVID-19.” (Photo copyright: Ellume.)
The Promise of Rapid Antigen COVID-19 Tests
In a column he wrote for Time in July, Ashish K. Jha, MD, MPH, a practicing General Internist and Dean of the Brown University School of Public Health, described the promise of rapid antigen tests. “Imagine spitting on a special strip of paper every morning and being told two minutes later whether you were positive for COVID-19,” he wrote. “If everyone in the United States did this daily, we would dramatically drop our transmission rates and bring the pandemic under control.”
Another advocate for this approach is Michael Mina, MD, PhD, an assistant professor of epidemiology at the Harvard T.H. Chan School of Public Health and a core member of the School’s Center for Communicable Disease Dynamics (CCDD). In a commentary for Time in November he wrote, “Widespread and frequent rapid antigen testing (public health screening to suppress outbreaks) is the best possible tool we have at our disposal today—and we are not using it.”
However, one major issue with antigen testing is sensitivity. “Antigen tests require higher levels of virus than qPCR [quantitative polymerase chain reaction] to return a positive result,” Jha wrote in Time. However, he contends, “the frequency of testing and the speed of results” counter concerns about accuracy.
Even with lower sensitivity, Jha wrote, the quicker test results from antigen tests “would identify viral loads during the most infectious period, meaning those cases we care most about identifying—at the peak period of infectiousness—are less likely to be missed.”
As the FDA explains, RT-PCR molecular tests “detect the virus’ genetic material,” whereas, according to an article published in Nature, titled, “Fast Coronavirus Tests: What They Can and Can’t Do,” antigen tests can “detect specific proteins … on the surface of the virus, and can identify people who are at the peak of infection, when virus levels in the body are likely to be high.”
At-Home Antigen Tests Receive EUAs
The new antigen test developed by Ellume is “the first over-the-counter (OTC) fully at-home diagnostic test for COVID-19,” the FDA said in a press release. The user self-administers a nasal swab and places it in an analyzer connected to a smartphone app. It can deliver results in 20 minutes. The company states that its test has overall sensitivity of 95% and specificity of 97% based on a clinical study of 198 subjects in a simulated home setting.
Jeffrey Shuren, MD, JD, Director of FDA’s Center for Devices and Radiological Health, said in the FDA press release, “This test, like other antigen tests, is less sensitive and less specific than typical molecular tests run in a lab. However, the fact that it can be used completely at home and return results quickly means that it can play an important role in response to the pandemic.”
Ellume expects to deliver about 20 million tests to the US by the end of June 2021. Multiple outlets reported that the test will cost about $30, AP News reported.
Meanwhile, the FDA also authorized at-home use of Abbott’s BinaxNOW rapid antigen test, which was previously authorized for use in point-of-care settings. This test, which requires a prescription, will sell for $25.
In a series of tweets, Harvard’s Mina applauded both moves, but he wrote that they [antigen tests] still fall short of his vision for fast and frequent testing. He described Abbott’s BinaxNOW as “the type of rapid test I have been calling for,” but said he’d like to see tests priced far less and available without a prescription.
Diminishing Prospects for Saliva-based Antigen Tests?
All rapid antigen tests authorized by the FDA so far require nasopharyngeal and/or nasal swab specimens, and it appears that it may be a long time, if ever, before saliva-based antigen tests are available. The New York Times (NYT) reported in October that two companies working on antigen tests—E25Bio and OraSure (NASDAQ:OSUR)—have dropped plans to enable use of saliva.
“If I was placing a bet—which I am, because I’m leading an antigen-based testing company—I would say it’s going to be very difficult for antigen-based testing to work on saliva samples,” E25Bio founder Bobby Brooke Herrera, PhD (above with E25Bio co-founder and Chief Technology Officer Irene Bosch) told the NYT. (Photo copyright: WCVB-TV.)
One advantage of a saliva-based test is that it would be easier to self-administer. “But as they continued to tinker with their tests, researchers at both E25Bio and OraSure found saliva’s performance to be more lackluster than anticipated, and were forced to pivot,” the New York Times reported. Instead, both companies will seek authorization for use of their tests with nasal swabs.
HHS Contract for Antigen Tests Brings High Rates of False Positives
A recent investigative story in ProPublica, titled, “Rapid Testing Is Less Accurate than the Government Wants to Admit,” raised additional questions about rapid antigen testing. In August, the US Department of Health and Human Services announced it had awarded a $760 million contract for 150 million Abbott BinaxNOW tests to be distributed to schools and nursing homes. But later, according to ProPublica, healthcare workers in Nevada and Vermont reported high rates of false positives.
“With the benefit of hindsight, experts said the Trump administration should have released antigen tests primarily to communities with outbreaks instead of expecting them to work just as well in large groups of asymptomatic people,” ProPublica reported. “Understanding they can produce false results; the government could have ensured that clinics had enough for repeat testing to reduce false negatives and access to more precise PCR tests to weed out false positives.”
A few weeks after the reports from Nevada and Vermont, the FDA issued a letter advising clinical laboratories and healthcare providers about the possibility of false positives, along with steps they could take to improve accuracy.
Though some experts remain hopeful about “fast-and-frequent” testing, others are skeptical and say more research is needed to assess the value of this approach. “We are open to thinking outside the box and coming up with new ways to handle this pandemic,” Esther Babady PhD, D(ABMM) of Memorial Sloan Kettering Cancer Center, told the New York Times. However, she added, “the data for that is what’s missing.”
Nevertheless, were at-home rapid saliva-based antigen tests to become a common choice for healthcare consumers, clinical laboratories that perform RT-PCR testing for COVID-19 could see a marked decrease in orders. Thus, regardless of the current state of antigen testing, its development is worth watching.
Clinical laboratory professionals should note that one case study describes a COVID-positive cancer patient shedding infectious particles for five months, which is much longer than expected
Just when researchers start believing they understand COVID-19 infections, something happens that reveals there is still more to learn. These additional findings are relevant for clinical laboratory managers and pathologists because the new insights often may play a role in how SARS-CoV-2 results should be interpreted for individual patients.
Researchers recently described a case where, in February, a 71-year-old woman underwent surgery related to her 10-year battle with cancer. While she was in the hospital, she was found to be positive for the SARS-CoV-2 coronavirus, though she showed no respiratory or systemic symptoms. Nevertheless, the hospital isolated her and monitored the infection.
To everyone’s surprise, the patient remained positive for five months. She underwent 15 COVID-19 tests from various diagnostics companies, as well as receiving two doses of convalescent plasma therapy, but she remained positive for the coronavirus into June.
In their published study, they wrote, “Although it is difficult to extrapolate from a single individual, our data suggest that long-term shedding of infectious virus may be a concern in certain immunocompromised people. Given that immunocompromised individuals could have prolonged shedding and may not have typical symptoms of COVID-19, symptom-based strategies for testing and discontinuing transmission-based precautions, as recommended by the Centers for Disease Control and Prevention (CDC), may fail to detect whether certain individuals are shedding infectious virus.”
Clinical laboratory professionals and pathologists will find it significant that patients with major health conditions may be shedding viral material for weeks longer than originally thought. This is relevant because it may be prudent to COVID test patients who present with compromised immune systems, and who are asymptomatic, and then repeat that testing at appropriate intervals.
The graphic above taken from the NIAID study shows how long it took for the SARS-CoV-2 coronavirus to clear the 71-year-old immunocompromised cancer patient’s system, and at which points the convalescent plasma doses were administered. (Graphic copyright: National Institute of Allergy and Infectious Diseases.)
Immunocompromised Patients May Handle COVID-19 Differently
The NIAID researchers believe the reason the patient continued to shed infectious virus for so long was because she was immunocompromised. They wrote, “Many current infection control guidelines assume that persistently PCR-positive individuals are shedding residual RNA and not infectious virus, with immunocompromised people thought to remain infectious for no longer than 20 days after symptom onset. Here we show that certain individuals may shed infectious, replication-competent virus for much longer than previously recognized. Although infectious virus could be detected up to day 70, sgRNA, a molecular marker for active SARS-CoV-2 replication, could be detected up until day 105.”
In the United States, some three million people have compromised or weakened immune systems. This is a significant population, Science Alert reported.
“As the virus continues to spread, more people with a range of immunosuppressing disorders will become infected, and it’s more important to understand how SARS-CoV-2 behaves in those populations,” Vincent Munster, PhD, Chief, Virus Ecology Unit at the National Institute of Allergy and Infectious Diseases and co-author of the NIAID study, told Science Alert.
The NIAID study findings match knowledge about other coronaviruses. For example, Science Alert reported that immunocompromised people with Middle East Respiratory Syndrome (MERS) have been shown to shed common seasonal coronaviruses for up to a month following infection.
That study included 303 patients, of which 193 were symptomatic. During the course of the study, 21 of the asymptomatic patients developed symptoms, however, the viral load was similar in all of the patients, regardless of symptoms.
“Isolation of asymptomatic patients may be necessary to control the spread of SARS-CoV-2,” concluded the JAMA researchers. But how long should asymptomatic patients remain isolated?
Official Guidance Is Based on Symptoms
The CDC updated its guidelines for who should isolate and for how long in October. The guidelines cover:
People who have or had COVID-19 and had symptoms;
People who tested positive for COVID-19 but did not have symptoms;
People who either had severe symptoms of COVID-19 or who have a compromised immune system;
People who were exposed to COVID-19, and
People who have been reinfected.
Regarding those who are immunocompromised and had COVID-19, the CDC says they “may require testing to determine when they can be around others.”
In addition to noting that people who are immunocompromised may require additional testing, the CDC is also continuously updating its published list of people who are at risk for complications and severe illness if they contract COVID-19. However, as the NIAID study showed, even those with underlying medical conditions can be asymptomatic.
And as the NIAID researchers note, there is more to learn. “Understanding the mechanism of virus persistence and eventual clearance will be essential for providing appropriate treatment and preventing transmission of SARS-CoV-2 because persistent infection and prolonged shedding of infectious SARS-CoV-2 might occur more frequently. Because immunocompromised individuals are often cohorted in hospital settings, a more nuanced approach to testing these individuals is warranted, and the presence of persistently positive people by performing SARS-CoV-2 gRNA and sgRNA analyses on clinical samples should be investigated.”
SARS-CoV-2 Science Is Young
An additional takeaway for pathology lab professionals is the reminder that the scientific research surrounding the novel coronavirus that causes COVID-19 is very young. New insights and understanding will continue to emerge, probably for many years.
One reason why the development of vaccines for COVID-19 has been so quick is that it built on scientific knowledge of the first SARS outbreak and MERS. It’s interesting to note that both SARS and MERS are relatively new as well: SARS emerged in 2002 and MERS in 2012. Compared to a disease like HIV, which was first identified in 1959, scientists have only been working on these particular coronaviruses for a short period of time.
The NIAID study is yet another example of new knowledge and insights emerging about how SARS-CoV-2 infects individuals. Collectively, these findings make it challenging for medical laboratory professionals to stay current with everything relevant and associated with the proper interpretation of COVID-19 test results.
Because air travel volumes are low, experts believe it is timely to develop COVID-19 testing systems and gain insight on which protocols are most effective
As the COVID-19 pandemic surges on, several international airlines now require customers to complete at-home COVID-19 testing before they can travel. This is triggering unusual business practices. For example, one airline allows its passengers to use frequent flier miles to purchase mail-in COVID-19 test kits.
Frequent Flyer Miles for COVID-19 Testing
Across the United States, Hawaii has one of the lowest rates of infection, partly thanks to the state’s strict quarantine regulations. In a state, however, that depends on tourism for its economic health, the pandemic has caused serious financial difficulties. In an effort to prevent spread of the coronavirus while also encouraging tourism, Hawaiian Airlines now offers “Pre-travel COVID-19 Test Options” on its website.
To be allowed to skip the state’s mandatory 14-day self-quarantine before arriving on the islands, flyers can take a pre-travel coronavirus test with the following conditions:
The test must be from a state-approved testing provider.
The test must be administered no more than 72 hours prior to the scheduled departure time of the final leg to Hawaii.
For trans-pacific travel, test results must be received prior to flight departure.
Additionally, the airline accepts frequent flyer miles to pay for mail-in COVID-19 tests. In exchange for 14,000 HawaiianMiles, a passenger receives a test kit in the mail. The kit features a video call during which a healthcare professional guides the consumer on taking a saliva sample. The user then ships the sample to a qualified clinical laboratory. Results are returned electronically within 24 hours of the lab receiving the sample.
Hawaii’s COVID-19 portal states, “The state of Hawaii will ONLY accept Nucleic Acid Amplification Test (NAAT) from a certified Clinical Laboratory Improvement Amendment (CLIA) lab test results from Trusted Testing and Travel Partners” that are participating in the state’s pre-travel testing program. Honolulu and Maui are the only two arrival airports allowed. A negative result must have come from a test performed within 72 hours prior to the final leg of the passenger’s trip to Hawaii, according to the portal.
“A negative pre-travel test is an alternative to two weeks in self-isolation for arrivals to the archipelago,” the UK’s Independent reported.
JetBlue and Vault Health Partner to Offer COVID Testing to Airline Passengers
In another instance of an airline getting involved in at-home testing, JetBlue (NASDAQ:JBLU) is partnering with Vault Health to offer at-home testing. The process is similar to the Hawaiian Airlines program. However, rather than purchasing the test with frequent flyer miles, JetBlue offers polymerase chain reaction (PCR) tests at a discount.
Business Travel News reported that passengers must provide a confirmation code while ordering the $119 test from Vault Health’s webpage. “Vault provides a kit for an at-home saliva test, and users administrate it while on a video chat supervised by Vault to ensure the test is done properly. The user sends it overnight to a clinical laboratory and the results are provided within 72 hours,” Business Travel News stated.
“We continue to hear from health officials that [COVID-19] testing is incredibly important in the fight against the coronavirus, and we want to make sure our customers have options for testing, especially prior to travel,” said Joanna Geraghty, President and Chief Operating Officer, JetBlue, in a press release. “As more and more regions reopen, many are requiring test results to enter. Now with easier testing options, those safety requirements may not be a deterrent for travel, but rather provide greater public health and peace of mind with little inconvenience.” (Photo copyright: Spectrum News NY1.)
In addition to airlines such as Hawaii Airlines and JetBlue instituting programs for coronavirus testing, some airports are as well. Tampa International Airport, for example, test-piloted a voluntary testing program for all arriving and departing passengers from October 1st to October 31st. The airport partnered with BayCare, a 15-hospital Tampa area healthcare network, to provide both rapid antigen and PCR tests.
“Testing services will be offered on a walk-in basis … seven days a week from 8 a.m. until 2 p.m. The pilot will be open to all ticketed passengers who are flying or have flown within three days and can show proof of travel. The PCR COVID-19 test costs $125 and the antigen test costs $57,” a press release stated.
Tampa Airport CEO Joe Lopano told the Washington Post, “This could be—especially if adopted by other airports—another way to instill confidence.”
COVID-19 Testing by Retailers Expanding as Well
Travelers aren’t the only people who need testing. Some employers also are requiring negative tests before employees can return to work.
As with all at-home kits, the consumer collects their own specimen and sends it off to a qualified clinical laboratory for processing. AZOVA, a telehealth company, supplies the kits to Costco for resale and provides a smartphone app where customers can check and display the test results.
P23 Labs’ TaqPath SARS-CoV-2 assay is the test being used, which, according to P23, “has a 98% sensitivity and 99% specificity,” Business Insider reported.
The researchers found that “All seven SARS-CoV-2 genomes were genetically identical, with the exception of a single mutation in one case, and all genomes had five signature mutations seen in only six other genomes from the >155,000 genomes sequenced globally. Four of these six related genome sequences were from Switzerland, the country of origin of the suspected index case.”
They added, “By combining information on disease progression, travel dynamics, and genomic analysis, we conclude that at least four in-flight transmission events of SARS-CoV-2 likely took place.”
At-home test kits for COVID-19 are here to stay. That large businesses in multiple industries are now partnering with COVID-19 test developers and clinical laboratory companies to accomplish testing of customers and employees means independent labs that process coronavirus testing can look forward to increasing COVID-19 testing business.
“We need to be using the time now, when [travel] volumes are relatively low, to test the systems and gain insight on which protocols are most effective,” Mara Aspinall, biomedical diagnostics professor at Arizona State University, President and CEO of the Health Catalysts Group, an investment and advisory firm, and former President/CEO of Ventana Medical Systems (now Roche Tissue Diagnostics), a billion-dollar division of Swiss pharmaceutical and diagnostics manufacturer Roche, told the Washington Post.
Researchers conducted antibody testing on ‘remainder plasma,’ which could inform strategies for ongoing SARS-CoV-2 clinical laboratory surveillance testing
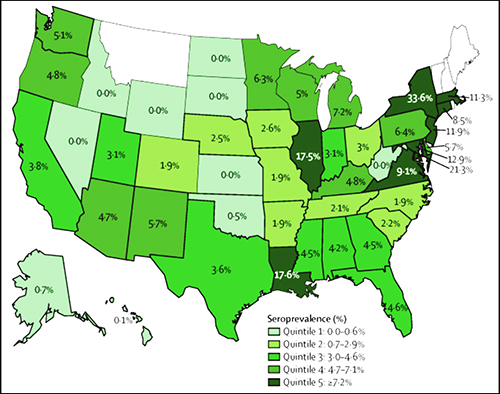
In a clever use of stored clinical laboratory specimens, researchers in California conducted a nationwide seroprevalence survey—serology testing to determine the number of people in a population that carry a specific disease—that used “remainder plasma” from dialysis patients to look for antibodies to the COVID-19 infection. They found that—as of July—fewer than one in 10 adults tested had acquired antibodies to the SARS-CoV-2 coronavirus.
According to Julie Parsonnet, MD, Stanford Professor of Medicine and of Epidemiology and Population Health, and a study author, this indicates that the US population is a long way from herd immunity to COVID-19. “This is the largest study to date to confirm that we are nowhere near herd immunity,” she said in a Stanford Medicine press release.
Herd immunity is the point at which a large part of the population becomes immune to a specific disease. Scientists, according to the Stanford press release, estimate that 60%-70% of the population must have antibodies to the coronavirus before COVID-19 fades.
The graphic above taken from Stanford Medicine’s published study illustrates the “prevalence of SARS-CoV-2 antibodies in sampled population, by state. Bolded borders represent states with more than 100 patients in the sample. The median number of patients sampled by state was 176 (IQR 83–536). States in white were not sampled.” (Graphic copyright: Stanford University.)
Dense Urban Populations at Greater Risk for COVID-19
The Stanford researchers analyzed samples of remainder plasma from 28,503 randomly selected patients receiving dialysis in July at more than 1,300 dialysis facilities in 46 states. They found that 8% of people were positive for COVID-19 antibodies, which when standardized to the US adult population, equals 9.3% nationwide, the study notes.
However, they also found that people living in densely populated areas were 10 times more likely to show evidence of past COVID-19 infection, and that people living in predominantly black and Hispanic neighborhoods were two to three times more likely to be seropositive than those in white neighborhoods, the researchers wrote.
Of the use of remainder plasma for their study, the researchers wrote, “Testing remainder plasma from monthly samples obtained for routine care of patients on dialysis for SARS-CoV-2 antibodies therefore represents a practical approach to a population-representative surveillance strategy, informing risks faced by a susceptible population while ensuring representation from racial and ethnic minorities.
“In addition, seroprevalence surveys in patients receiving dialysis can be linked to patient-level and community-level data to enable evaluation and quantification of differences in SARS-CoV-2 prevalence by demographic and neighborhood strata, and thus facilitate effective mitigation strategies targeting the highest-risk individuals and communities,” added the researchers.
When standardized to the US dialysis population, seroprevalence ranged from 3.5% (95% CI, 3.1-3.9) in the West to 27.2% (95% CI, 25.9-28.5) in the Northeast.
Large variations in seroprevalence by state were seen, with early COVID-19 hot spots such as New York (33.6%), Louisiana (17.6%), and Illinois (17.5%) having higher rates than neighboring states—Pennsylvania (6.4%), Arkansas (1.9%), and Missouri (1.9%).
When compared with other measures of SARS-CoV-2 spread, seroprevalence correlated best with deaths per 100,000 population.
“With this survey, we were able to provide a very rich picture of the first wave of the COVID-19 outbreak in the U.S. that can hopefully help inform strategies to curb the epidemic moving forward by targeting vulnerable populations,” said Shuchi Anand, MD (above left, with fellow Nephrologists Colin Lenihan and Michelle O’Shaughnessy), Director of Stanford’s Center for Tubulointerstitial Kidney Disease and lead author of the study. (Photo copyright: Stanford Medicine.)
Nearly 10% of COVID-Positives Are Undiagnosed
In another important finding that compared seroprevalence and case counts per 100,000 population as of June 15, the study reports that only 9.2% of the COVID-19 seropositives had been diagnosed with the disease.
Because dialysis patients get monthly laboratory blood tests that generate leftover blood plasma samples, researchers believe this remainder plasma can serve an important role in tracking COVID-19’s prevalence in the general population.
“Not only is this patient population representative of the US population, but they are one of the few groups of people who can be repeatedly tested,” said Anand in the Stanford press release. “This is a potential strategy for ongoing SARS-CoV-2 antibody testing and surveillance.”
“Questions remain around the longevity of the immune response and correlates of protection, but high-quality longitudinal serosurveillance with accompanying clinical data can help to provide the answers,” they wrote. “Anand and colleagues deserve credit for pioneering a scalable sampling strategy that offers a blueprint for standardized national serosurveillance in the USA and other countries with a large haemodialysing population.”
Pandemic Fatigue and the Vaccine
While the promised vaccine provides hope for an end to the pandemic, experts say the battle is far from won.
“We are still in the middle of the fight,” epidemiologist Eli Rosenberg, PhD, Associate Professor at the University at Albany in New York, who was not part of the Stanford study, told the Washington Post, “We’re all tired, and we’re all hoping for a vaccine. This shows us how it’s not over here, not even by a long shot.”
What is obvious is that clinical laboratories will continue to play a vital role in response to the COVID-19 pandemic. In fact, just as the management and scientific team at Ascend Clinical Laboratories recognized that remainder plasma from testing dialysis patients could be the foundation of a national seroprevalence survey for COVID-19, other clinical laboratories in different regions of the United States may have similar resources that can be adapted as tools to study and understand the SARS-CoV-2 pandemic.