Clinical laboratory managers and pathology practice administrators should consider how these trends may affect their business and patients when planning for the future.
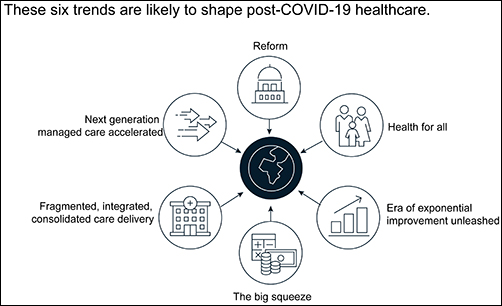
The McKinsey graphic above illustrates the “six trends that are likely to shape post-COVID-19 healthcare.” Clinical laboratories that support health networks struggling with any of these challenges should take steps to prepare for anticipated changes to healthcare delivery. (Graphic copyright: McKinsey and Company.)
1: Healthcare Reform
McKinsey identified three areas where the coronavirus pandemic may impact healthcare reform:
“COVID-19-era waivers that could become permanent.
“Actions that may be taken to strengthen the healthcare system to deal with pandemics.
“Reforms to address the COVID-19-induced crisis.”
McKinsey reports that “the Centers for Medicare and Medicaid Services has introduced more than 190 waivers since the beginning of March 2020.” These waivers can affect all aspects of healthcare, from clinical practice to reimbursement. Some of them, according to McKinsey, are “only relevant during the crisis (for example, the waiver of intensive care unit death reporting). A retrospective assessment of others (for example, expansion of telehealth access) could reveal beneficial innovation worth preserving.”
Several areas that McKinsey says are clearly ripe for reform include improving the resiliency of the healthcare system and the way the system is funded.
Public sector budgets are generally kept strictly separate, each with its own rules and policies that dictate operations. But in his article, “After COVID-19—Thinking Differently About Running the Health Care System,” published in JAMA Health Network, Stuart M. Butler, PhD, Senior Fellow in Economic Studies at the Brookings Institution, wrote, “The intensity of the COVID-19 pandemic … is forcing jurisdictions all across the country to find ways to be nimble so that multiple agencies can work together.”
Thus, McKinsey recommends, “Given the substantial shifts in relative market positioning among industry players that prior reforms have created, leaders would do well to plan ahead now.”
2: Better Access to Healthcare Services
Some people who develop COVID-19 are at far greater risk of hospitalization and death than others, including those who have:
Chronic health conditions, including obesity.
Mental and behavioral health challenges, such as substance abuse.
Unmet social needs, such as food or housing insecurity.
Poor access to healthcare.
McKinsey wrote that these “intersecting health and social conditions,” combined with certain races that have higher risk for severe complications, including Black, Indian, and Hispanic/Latino Americans, “correlated with poorer health outcomes.”
Value-based healthcare, telehealth, and greater attention to the social determinants of health may help address some of these issues, McKinsey notes, but the pandemic has shined a spotlight on how lack of care increases risk for certain populations during a public health crisis.
3: Era of Exponential Improvement Unleashed
Some of the trends that appear to be accelerating as a result of the pandemic are good news. McKinsey cites several benefits, including:
Improved understanding of patients.
Delivery of more convenient and individualized care.
$350-$410 billion in annual revenue by 2025.
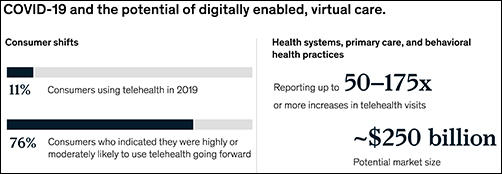
Through telehealth and other types of virtual care enabled by digital technology, “intuitive healthcare ecosystems” may arise and offer a more integrated experience for patients and their caregivers, McKinsey notes.
“While the pace of change in healthcare has lagged other industries in the past, potential for rapid improvement may accelerate due to COVID-19. An example is the exponential uptake of digitally enabled, virtual care,” McKinsey wrote. “Our analysis … showed that health systems, primary care, and behavioral health practices are reporting increases of more than 50–175 times in telehealth visits, and the potential market size for virtual care could reach around $250 billion.”
The graphic above is taken from the McKinsey and Co. report, which noted, “Proliferation of digitally enabled, virtual care could further contribute to the rise of personalized and intuitive healthcare ecosystems [that] have the potential to deliver an integrated experience to consumers, enhance productivity of providers, engage both formal and informal caregivers, and improve outcomes while lowering cost.” (Graphic copyright: McKinsey and Company.)
4: The Big Squeeze
The pandemic has caused an enormous outflow of cash from the healthcare system, and some experts don’t expect an injection of funding until 2022. “This outflow is expected to be primarily driven by coverage shifts out of employer-sponsored insurance and possible coverage reductions by employers as well as Medicaid rate pressures from states,” McKinsey states.
“We estimate that COVID-19 could depress healthcare industry earnings by between $35 billion and $75 billion compared with baseline expectations,” McKinsey predicted, adding, “Select high-growth segments will remain attractive (for example, virtual care, home health, software and platforms, specialty pharmacy) and will disproportionally drive growth. These high-growth areas are expected to increase more than 10% over the next five years, while other segments may stagnate or decline altogether.”
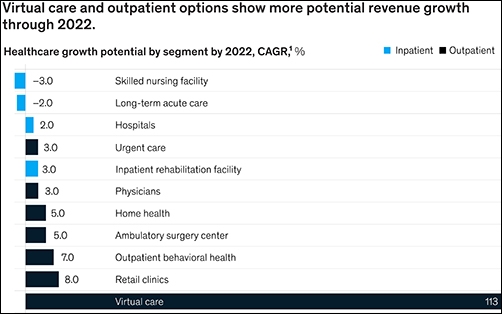
5: Fragmented, Integrated, Consolidated Care Delivery
McKinsey says, “The shift of care out of hospitals is not new but has been accelerated by COVID-19.” Rather than the hospital being the center of care delivery, patients are increasingly choosing to receive care at a range of sites across many healthcare ecosystems that are connected digitally and through analytics.
Early in the course of the pandemic, visits to ambulatory care facilities dropped nearly 60% by early April. But by mid-May, those visits were beginning to rebound.
In, “The Impact of the COVID-19 Pandemic on Outpatient Visits: A Rebound Emerges,” the Commonwealth Fund reported that “the relative decline in visits remains largest among surgical and procedural specialties and pediatrics” but is “smaller in other specialties, such as adult primary care and behavioral health.”
The McKinsey graphic above shows how “virtual care and outpatient options show more potential revenue growth through 2022.” Clinical laboratories that support those healthcare settings, especially ambulatory surgery, behavioral health, and retail clinics, should experience similar growth. (Graphic copyright: McKinsey and Company.)
6: Adoption of Next-Generation Managed Care Is Accelerating
How will COVID-19 affect the managed care industry? McKinsey says the “next generation” of managed care might use Medicare Advantage as a model.
“Payers pursuing the next generation of managed care model (through deep integration with care delivery) demonstrate better financial performance, capturing an additional 50 basis points of earnings before interest, taxes, depreciation, and amortization above expectation,” McKinsey noted, adding, “Employers and payers could consider fundamentally rethinking how employer-sponsored health coverage is structured. Learning from Medicare Advantage could provide inspiration for such a reimagination.”
What Should Clinical Laboratory Managers Do?
The McKinsey article concludes by stating, “While the challenges are numerous, leaders who seize the mindset that “disruptive change provides an opportunity to separate yourself from the pack” will build organizations meaningfully stronger than the ones they ran going into the crisis.”
The McKinsey article authors recommend that healthcare organizations take several proactive steps, including:
Launch a plan-ahead team.
Question your role and your future business model.
Prepare to transform your business.
Reimagine your organization to make faster decisions.
Take action to drive health equity.
Though the McKinsey and Company article covered healthcare in general, many of the authors’ observations and recommendations can apply to clinical laboratories and pathology groups as well and may be valuable in future planning.
Critical shortages in medical laboratory workers and supplies are yet to be offset by new applicants and improved supply chains. But there is cause for hope.
Medical laboratory scientists (aka, medical technologists) can be hard to find and retain under normal circumstances. During the current coronavirus pandemic, that’s becoming even more challenging. As demand for COVID-19 tests increases, clinical laboratories need more technologists and lab scientists with certifications, skills, and experience to perform these complex assays. But how can lab managers find, attract, and retain them?
The Johns Hopkins Coronavirus Resource Center reports that as of mid-October more than one million tests for SARS-CoV-2 were being performed daily in the US. And as flu season approaches, the pandemic appears to be intensifying. However, supply of lab technologists remains severely constrained, as it has been for a long time.
Still, qualified medical technologists (MT) and clinical laboratory scientists (CLS) are hard to find.
Demand for COVID Tests Exceeds Available Clinical Lab Applicants
“I can replace hardware and I can manage not having enough reagents, but I can’t easily replace a qualified [medical] technologist,” said David Grenache, PhD, Chief Scientific Officer at TriCore Reference Laboratories, Albuquerque, N.M., in the WSJ.
Another area where demand outstrips supply is California. Megan Crumpler, PhD, Laboratory Director, Orange County Public Health Laboratory, told the WSJ, “We are constantly scrambling for personnel, and right now we don’t have a good feel about being able to fill these vacancies, because we know there’s not a pool of applicants.”
Are Reductions in Academic Programs Responsible for Lack of Available Lab Workers?
Recent data from the US Bureau of Labor Statistics (BLS) show 337,800 clinical laboratory technologists and technicians employed by hospitals, public health, and commercial labs, with Job Outlook (projected percent change in employment) growing at 7% from 2019 to 2029. This, according to the BLS’ Occupational Outlook Handbook on Clinical Laboratory Technologists and Technicians, is “faster than average.”
“The average growth rate for all occupations is 4%,” the BLS notes.
Medical laboratories have the most staff vacancies in phlebotomy (13%) and the least openings in point-of-care (4%), according to an American Society for Clinical Pathology 2018 Vacancy Survey published in the American Journal of Clinical Pathology (AJCP).
Becker’s Hospital Review reported that “Labor shortages in [clinical] testing labs have existed for years due to factors including low recruitment, an aging workforce, and relatively low pay for [medical] lab technicians and technologists compared to that of other healthcare workers with similar education requirements.
“In 2019, the median annual salary for clinical laboratory technologists and technicians was $53,000, according to the US Bureau of Labor Statistics. The skills required for lab workers also are often specialized and not easily transferred from other fields.”
At the “root” of the problem, according to an article in Medical Technology Schools, is a decrease in available academic programs. Laboratory technologists require a Bachelor of Science (BS) degree and technicians need an associate degree or post-secondary certificate.
“(The programs) are expensive to offer, so when it comes to cuts and budgets, some of those cuts have been based on how much it costs to run them. That, and they may not have high enough enrollments,” said Lisa Cremeans, MMDS, CLS(NCA), MLS(ASCP), Clinical Assistant Professor at University of North Carolina at Chapel Hill, in the Medical Technology Schools article. (Photo copyright: University of North Carolina.)
AACC has called for federal funding of these programs, which now number 608, down from 720 programs for medical laboratory scientists in 1990.
“The pandemic has shone a spotlight on how crucial testing is to patient care. It also has revealed the weak points in our country’s [clinical laboratory] testing infrastructure, such as the fact that the US has allowed the number of laboratory training programs to diminish for years now,” said Grenache, who is also AACC President, in a news release.
Creative Staffing Strategies Clinical Labs Can Take Now
select “apply code” and complete the registration.
How Some Clinical Labs are Coping with Staff and Recruitment Challenges
The Arizona Chamber Business News reported that Sonora Quest Laboratories in Tempe earlier this year launched “Operation Catapult” to help with a 60,000 COVID-19 test increase in daily test orders. The strategy involved hiring 215 employees and securing tests with the help of partners:
Meanwhile, students in the UMass Lowell (UML) medical laboratory science (MLS) program, see brighter skies ahead.
“The job outlook even before COVID-19 was so amazing,” said Dannalee Watson, a UML MLS student, in a news release. “It’s like you’re figuring out a puzzle with your patient. Then, we help the doctor make decisions.”
Such enthusiasm is refreshing and reassuring. In the end, the SARS-CoV-2 pandemic and the resultant demand for clinical laboratory testing may call more students’ attention to careers in medical laboratories and actually help to solve the lab technologist/technician shortage. We can hope.
About 50% of South Asians and 16% of Europeans carry gene cluster associated with respiratory failure after SARS-CoV-2 infection and hospitalization
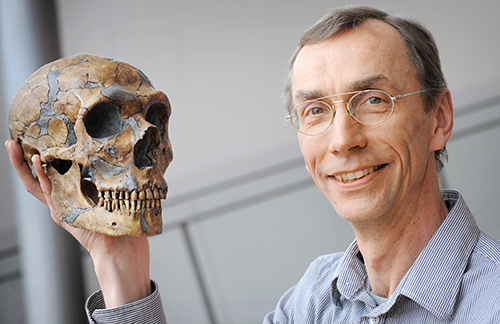
Clinical pathology laboratories and medical laboratory scientists may be intrigued to learn that scientists from two research institutes in Germany and Sweden have determined that a strand of DNA associated with a higher risk of severe COVID-19 in humans is similar to the corresponding DNA sequences of a roughly 50,000-year-old Neanderthal from Croatia.
The researchers concluded that this gene cluster—passed down from Neanderthals to homo sapiens—triples the risk of developing severe COVID-19 respiratory symptoms for some modern day humans.
In a press release, Pääbo said, “It is striking that the genetic heritage from the Neanderthals has such tragic consequences during the current pandemic. Why this is must now be investigated as quickly as possible.”
Might Useful Biomarkers for Clinical Laboratory Tests Be Identified?
Though it is not immediately clear how these findings may alter current approaches to developing treatments and a vaccine for the SARS-CoV-2 coronavirus, it is another example of how increased knowledge of human DNA leads to new understandings about genetic sequences that can spur development of useful biomarkers for clinical laboratory diagnostics tests.
Swedish geneticist Svante Pääbo, PhD (above right), Director of the Max Planck Institute for Evolutionary Anthropology in Germany, is co-author of a recent study that traced a gene cluster linked to a higher risk of severe COVID-19 to 50,000-year-old Neanderthals from Croatia. “It is striking that the genetic heritage from the Neanderthals has such tragic consequences during the current pandemic,” he said. Nevertheless, such discoveries sometimes lead to new biomarkers for clinical laboratory tests and diagnostics. (Photo copyright: Max Planck Institute for Evolutionary Anthropology.)
This latest research reveals that people who inherit a specific six-gene combination on chromosome 3—called a haplotype—are three times more likely to need artificial ventilation if they are infected by the SARS-CoV-2 coronavirus. Yet, the researchers can only speculate as to why the gene cluster confers a higher risk.
“The genes in this region may well have protected the Neanderthals against some other infectious diseases that are not around today. And now, when we are faced with the [SARS-CoV-2] coronavirus, these Neanderthal genes have these tragic consequences,” Pääbo told the Guardian.
According to the study, the gene risk variant is most common in South Asia where about half of the population carries the Neanderthal risk variant. In comparison, one in six Europeans have inherited the gene sequence and the trait is almost nonexistent in Africa and East Asia.
“About 63% of people in Bangladesh have at least one copy of the disease-associated haplotype, and 13% have two copies (one from their mother and one from their father). For them, the Neandertal DNA might be partially responsible for increased mortality from a coronavirus infection. People of Bangladeshi origin living in the United Kingdom, for instance, are twice as likely to die of COVID-19 as the general population,” Science News reported.
Other Research Connecting Genes to Severe COVID-19 Symptoms
The haplotype on chromosome 3 first made headlines in June when the New England Journal of Medicine (NEJM) published the “Genomewide Association Study of Severe COVID-19 with Respiratory Failure,” which analyzed COVID-19 patients in seven hospitals in Italy and Spain. The researchers found an association between the gene cluster on chromosome 3 and severe symptoms of SARS-CoV-2 after infection and hospitalization. The study also pointed to the potential involvement of chromosome 9, which contains the ABO blood-group system gene, indicating that humans with type A blood may have a 45% higher risk of developing severe COVID-19 infections.
However, Mark Maslin, PhD, Professor of Climatology at University College London, cautions against drawing strong conclusions from the initial research tying disease risk to the genetic legacy of Neanderthals, the Guardian reported. He suggested that, while the Neanderthal-derived variant may contribute to COVID-19 risk in certain populations, genes are more likely to be just one of multiple risk factors for COVID-19 that include age, gender, and pre-existing conditions.
“COVID-19 is a complex disease, the severity of which has been linked to age, gender, ethnicity, obesity, health, virus load among other things,” Maslin told the Guardian. “This paper links genes inherited from Neanderthals with a higher risk of COVID-19 hospitalization and severe complications. But as COVID-19 spreads around the world it is clear that lots of different populations are being severely affected, many of which do not have any Neanderthal genes.
“We must avoid simplifying the causes and impact of COVID-19, as ultimately a person’s response to the disease is about contact and then the body’s immunity response, which is influenced by many environmental, health and genetic factors.”
Andre Franke, PhD, Director of the Institute of Clinical Molecular Biology, Kiel University in Germany, agrees with Maslin, the Associated Press reported. In a statement “ahead of the study’s final publication,” he said these latest findings have no immediate impact on the treatment of COVID-19, and he questioned “why that haplotype—unlike most Neanderthal genes—survived until today,” AP reported.
All of this deepens the mystery of the SARS-CoV-2 coronavirus. Genomics research continues to add new insights into what is known about COVID-19 and may ultimately provide answers on why some people contract the disease and remain asymptomatic—or have mild symptoms—while others become seriously ill or die. Understanding why and how certain genes increase the risk of severe COVID-19 could give rise to targeted clinical laboratory tests and therapies to fight the disease.
Clinical laboratory managers may want to follow the debate that surfaced shortly after publication of the study in a peer-reviewed journal, when editors of the journal issued concerns over the researchers’ claims
Virologists and medical laboratory scientists continue to investigate ways the SARS-CoV-2 coronavirus can be defeated using the body’s own defenses in conjunction with medical treatments and a possible vaccine. Now, researchers at the Boston University School of Medicine have discovered that higher levels of vitamin D in the blood may improve chances of recovering from a COVID-19 infection.
“This study provides direct evidence that Vitamin D sufficiency can reduce the complications, including the cytokine storm (release of too many proteins into the blood too quickly) and ultimately death from COVID-19,” Michael F. Holick, PhD, MD, Professor of Medicine, Physiology and Biophysics at Boston University School of Medicine and one of the authors of the study, told SciTechDaily.
Holick is well-known in the scientific community for his many published studies on Vitamin D. In 2018, Kaiser Health News and The New York Times published a retrospective on Holick and his advocacy on behalf of Vitamin D, titled, “The Man Who Sold America On Vitamin D—and Profited in the Process.” In that story, Holick acknowledged working as a consultant for several organizations, including Quest Diagnostics in a relationship that dates back to 1979. KHN and NYT noted that Quest Diagnostics performs Vitamin D tests.
The Boston University researchers published their study in PLOS ONE, a peer-reviewed open-access scientific journal published by the Public Library of Science (PLOS). The paper’s apparent conclusions, however, invoked an “expression of concern” from the journal’s editors, which, along with direct responses from the Boston University researchers, can be read on PLOS ONE.
Can Vitamin D Save Lives?
To perform their research, the Boston University researchers examined the Vitamin D levels of 235 patients who had been admitted to a hospital with a SARS-CoV-2 infection. The patients were then tracked for clinical outcomes, including:
Blood samples were also analyzed for the number of lymphocytes and inflammatory markers. The researchers compared the collected data between patients who were sufficient to those who were deficient in Vitamin D levels.
They determined that patients over the age of 40 who were Vitamin D sufficient were 51.5% less likely to die from a COVID-19 infection than those who were deficient in the vitamin.
“Because Vitamin D deficiency and insufficiency is so widespread in children and adults in the United States and worldwide, especially in the winter months, it is prudent for everyone to take a vitamin D supplement to reduce risk of being infected and having complications from COVID-19,” Michael F. Holick, PhD, MD (above), told SciTechDaily. The Boston University School of Medicine professor and study author has been praising the health benefits of Vitamin D for years. He played a role in drafting national guidelines for the vitamin and also authored books that tout the advantages of Vitamin D, the importance of UV rays, and the biologic effects of light. (Photo copyright: Boston Herald.)
How Vitamin D Works and Why It’s So Important
In a fact sheet, the National Institutes of Health (NIH) recommend that adults between the ages of 19 and 70 take 15 micrograms (mcg) or 600 International Units (IU) of Vitamin D per day. Adults over the age of 70 should increase that amount to 20 mcg or 800 IUs per day.
According NBC News, Americans spent $936 million on supplements in 2017, which was nine times more than the previous decade. That article also stated that medical laboratory testing for Vitamin D levels have exponentially increased over the years. More than 10 million tests for Vitamin D levels were ordered for Medicare patients in 2016 at a cost of $365 million, which represents an increase of 547% since 2007. Currently, approximately one in four adults over the age of 60 in the US take Vitamin D supplements.
The NIH fact sheet notes that Vitamin D is a nutrient found in cells throughout the body and is needed for good health and to maintain strong bones. Individuals who are deficient in Vitamin D may develop soft, thin, brittle bones, as well as rickets in children and osteomalacia in adults. Vitamin D also helps the immune system fight off invading bacteria and viruses, helps nerves carry messages between the brain and other body parts, and helps muscles move. It can also play a role in warding off osteoporosis in older adults.
Very few foods naturally contain Vitamin D. The best dietary sources for the vitamin are fatty fish such as salmon, tuna, and mackerel, and foods fortified with Vitamin D, such as milks, some breakfast cereals, and yogurt. Being outside on sunny days is another way to obtain Vitamin D, as the body makes the vitamin when skin is directly exposed to the sun.
The Boston University study outlines the advantages of having sufficient Vitamin D levels, as well as how the vitamin may help ward off and possibly lessen the effects of infections like COVID-19, though those conclusions have been called into question.
Nevertheless, individuals who are deficient in the vitamin may want to take a supplement or get plenty of sunshine, just to be on the safe side. And clinical laboratory managers will want to keep in mind that over the years “the steady increase in physician and patient demand for Vitamin D tests has kept most clinical and pathology laboratories scrambling to maintain turnaround times and quality,” which Dark Daily reported in “Why Vitamin D Continues to Be the World’s Fastest-Growing Clinical Laboratory Test.”
CEOs of NorDx Laboratories, Sonora Quest Laboratories, and HealthPartners/Park Nicollet Laboratories expect demand for SARS-CoV-2 tests to only increase in coming months
The short answer is that large volumes of COVID-19 testing will be needed for the remaining weeks of 2020 and substantial COVID-19 testing will occur throughout 2021 and even into 2022. This has major implications for all clinical laboratories in the United States as they plan budgets for 2021 and attempt to manage their supply chain in coming weeks. The additional challenge in coming months is the surge in respiratory virus testing that is typical of an average influenza season.
Stan Schofield (above center), President of NorDx, a regional laboratory corporation that supports an integrated delivery system at MaineHealth in Portland, Maine.
Rick L. Panning (above right), MBA, MLS(ASCP)CM, retired as of Oct. 2 from the position of Senior Administrative Director of Laboratory Services for HealthPartners and Park Nicollet in Minneapolis-St. Paul, Minnesota.
Each panelist was asked how his parent health system and clinical laboratory was preparing to respond to the COVID-19 pandemic through the end of 2020 and into 2021.
First to answer was Panning, whose laboratory serves the Minneapolis-Saint Paul market.
A distinguishing feature of healthcare in the Twin Cities is that it is at the forefront of operational and clinical integration. Competition among health networks is intense and consumer-focused services are essential if a hospital or physician office is to retain its patients and expand market share.
Panning first explained how the pandemic is intensifying in Minnesota. “Our state has been on a two-week path of rising COVID-19 case numbers,” he said. “That rise is mirrored by increased hospitalizations for COVID-19 and ICU bed utilization is going up dramatically. The number of hospitalized COVID-19 patients has doubled during this time and Minnesota is surrounded by states that are even in worse shape than us.”
These trends are matched by the outpatient/outreach experience. “We are also seeing more patients use virtual visits to our clinics, compared to recent months,” noted Panning. “About 35% of clinical visits are virtual because people do not want to physically go into a clinic or doctor’s office.
“Given these recent developments, we’ve had to expand our network of specimen collection sites because of social distancing requirements,” explained Panning. “Each patient collection requires more space, along with more time to clean and sterilize that space before it can be used for the next patient. Our lab and our parent health system are focused on what we call crisis standards of care.
“For all these reasons, our planning points to an ongoing demand for COVID-19 testing,” he added. “Influenza season is arriving, and the pandemic is accelerating. Given that evidence, and the guidance from state and federal officials, we expect our clinical laboratory will be providing significant numbers of COVID-19 tests for the balance of this year and probably far into 2021.”
COVID-19 Vaccine Could Increase Antibody and Rapid Molecular Testing
Arizona is seeing comparable increases in new daily COVID-19 cases. “There’s been a strong uptick that coincides with the governor’s decision to loosen restrictions that allowed bars and exercise clubs to open,” stated Dexter. “We’ve gone from a 3.8% positivity rate up to 7% as of last night. By the end of this week, we could be a 10% positivity rate.”
Looking at the balance of 2020 and into 2021, Dexter said, “Our lab is in the midst of budget planning. We are budgeting to support an increase in COVID-19 PCR testing in both November and December. Arizona state officials believe that COVID-19 cases will peak at the end of January and we’ll start seeing the downside in February of 2021.”
The possible availability of a SARS-CoV-2 vaccine is another factor in planning at Dexter’s clinical laboratory. “If such a vaccine becomes available, we think there will be a significant increase in antibody testing, probably starting in second quarter and continuing for the balance of 2021. There will also be a need for rapid COVID-19 molecular tests. Today, such tests are simply unavailable. Because of supply chain difficulties, we predict that they won’t be available in sufficient quantities until probably late 2021.”
COVID-19 Testing Supply Shortages Predicted as Demand Increases
At NorDx Laboratories in Portland, Maine, the expectation is that the COVID-19 pandemic will continue even into 2022. “Our team believes that people will be wearing masks for 18 more months and that COVID-19 testing with influenza is going to be the big demand this winter,” observed Schofield. “The demand for both COVID-19 and influenza testing will press all of us up against the wall because there are not enough reagents, plastics, and plates to handle the demand that we see building even now.
“Our hospitals are already preparing for a second surge of COVID-19 cases,” he said.
COVID-19 patients will be concentrated in only three or four hospitals. The other hospitals will handle routine work. Administration does not want to have COVID-19 patients spread out over 12 or 14 hospitals, as happened last March and April.
“Administration of the health system and our clinical laboratory think that the COVID-19 test volume and demand for these tests will be tough on our lab for another 12 months. This will be particularly true for COVID-19 molecular tests.”
As described above, the CEOs of these three major clinical laboratories believe that the demand for COVID-19 testing will continue well into 2021, and possibly also into 2022. A recording of the full session was captured by the virtual Executive War College and, as a public service to the medical laboratory and pathology profession, access to this recording will be provided to any lab professional who contacts info@darkreport.com and provides their email address, name, title, and organization.
Robert L. Michel, Panelist—Publisher, Editor-in-Chief, The Dark Report and Dark Daily, Spicewood, Texas.
Given the importance of sound strategic planning for all clinical laboratories and pathology groups during their fall budget process, the virtual Executive War College is opening this session to all professionals in laboratory medicine, in vitro diagnostics, and lab informatics.