Since the pandemic began, federal investigators are specifically looking for patterns of fraud in Medicare claims data for COVID-19 clinical laboratory testing
Last month, the federal Department of Health and Human Services (HHS) Office of Inspector General (OIG) announced it had been investigating trends in Medicare claims data that could indicate patterns of fraud in the billing for COVID-19 clinical laboratory tests, Modern Healthcare reported.
Stretching back to at least March, fraudulent actors offering fake SARS-CoV-2 tests have preyed on vulnerable Americans in a wide variety of ways during the public health emergency, according to published reports. Some scam operators have gone into nursing homes and long-term care facilities to collect cash from unsuspecting elders in exchange for swab collections and phony testing, the New York Times reported.
Since the declaration of the public health emergency in the US, the federal Centers for Medicare and Medicaid Services (CMS) no longer requires a lab test requisition signed by a treating physician or other provider for COVID-19 testing. “The strong demand for and limited supply of SARS-CoV-2 tests, along with the move by CMS to relax rules for certain test orders during the pandemic, makes the situation a potentially ripe one for fraud,” Modern Healthcare stated.
Plus, a lack of clarity about the medical necessity of COVID-19 tests could raise the liability risk for law-abiding clinical laboratories. All of these factors make COVID-19 testing fraud a potential bombshell for clinical laboratories conducting coronavirus testing that may get caught up in federal investigations.
Feds Step Up Enforcement
Shortly after the pandemic arrived in the US, the FBI, the Better Business Bureau (BBB), the FDA, the federal Department of Health and Human Services (HHS), and other federal and local authorities have frequently warned doctors, hospitals, and healthcare consumers about the potential for fraud by unscrupulous companies purporting to offer legitimate clinical laboratory testing for COVID-19. A June 26 FBI press release stated, “Scammers are marketing fraudulent and/or unapproved COVID-19 antibody tests, potentially providing false results.”
Some of the fraudsters behind these scams have operated online and through social media and email. While others have conducted these scams in person or over the phone, noted the press release.
And yet, despite the warnings, the scams and news articles about them have continued to spread throughout the COVID-19 pandemic.
Various Forms of Fraud and Their Consequences
In many of these scams, fraudsters seek to collect consumers’ personal information, including names, dates of birth, and Social Security numbers, as well as other forms of personal health information, such as Medicare or private health insurance data, the FBI reported. Scammers can use that information in medical insurance fraud schemes or to commit identity theft, the agency added.
Additionally, any fake or inaccurate COVID-19 tests or assays that the FDA has not allowed for use could provide doctors with false results, potentially creating a dangerous situation for patients.
The New York Times (NYT) recently reported that the FBI had issued a warning “about scammers who advertise fraudulent COVID-19 antibody tests as a way to obtain personal information that can be used for identity theft or medical insurance fraud.”
Three days after the FBI issued its warning about the COVID-19 antibody testing scam, the BBB added an alert to its website: “BBB Scam Alert: Want a COVID-19 test? There’s a scam for that.” BBB also provided advice to consumers about how to avoid testing scams.
On June 17, the FDA reported that it issued warning letters to three companies for marketing adulterated and misbranded COVID-19 antibody tests, stated an FDA news release. The agency sent warning letters to:
In the FDA’s announcement, Jeff Shuren, MD, JD (above), Director of the FDA’s Center for Devices and Radiological Health, said “When tests are marketed inappropriately, with inaccurate or misleading claims—such as the ability to perform the test completely at home, or that the test is authorized, cleared, or approved when it is not—they put the health of Americans at risk. Such conduct will not be tolerated by the FDA, and we will continue to monitor tests marketed in the US, taking appropriate action as warranted.” (Photo copyright: The Food and Drug Administration.)
Scams Reported Just in April
On April 17, the New York Times reported that a special agent with the HHS OIG noted that impostors seeking Medicare or Medicaid information posed as doctors or laboratory technicians to offer fake tests in nursing homes and assisted living facilities.
Earlier in April, The Texas Tribune reported that the owner of a freestanding emergency room in Laredo, Texas, spent $500,000 to buy 20,000 rapid COVID-19 tests for patients suspected of having COVID-19. Health officials in Laredo planned to establish a drive-through testing site and then administer tests that came from a manufacturer in China to detect active infections. After trying to validate the tests, city health officials found they were unreliable and unusable.
An April 9 report from the news department of the AARP (American Association of Retired Persons) stated that federal officials have found fake coronavirus testing sites in many states, including Alabama, Arizona, Florida, Georgia, Kentucky, New York, and Washington state.
The FBI, according to AARP, investigated several fake test sites in Louisville, Ky., after a city official reported that people in personal protective equipment (PPE) were collecting biological specimens from residents. Those seeking tests were told to pay $240 in cash or give their Medicare, Medicaid, or Social Security cards to verify their identity.
Fake drive-up testing sites were reported at gas stations and other locations in Louisville over a four-day period, the AARP reported.
On April 2, WRGB TV in Albany, N.Y., reported that scammers pretending to be from the New York State Department of Health (NYSDOH) were taking money and insurance information from people in exchange for fake coronavirus tests. One woman told police she got a fake test at a drive-up site in a Little League parking lot.
North Greenbush police said the scammers identified themselves as being with NYSDOH and collected money and insurance information from multiple people. Police and state officials said the DOH had no connection to the collection site in the parking lot.
Lessons for Lab Directors
For clinical laboratory directors and all clinical lab scientists, the lesson from these stories is to be wary of strangers offering COVID-19 testing, while also making certain to post information for customers about the legitimacy of your lab’s COVID-19 rapid molecular and serological tests. Doing so might involve providing proof that the FDA has allowed your tests to be used for the coronavirus.
Also, medical laboratories should ensure that all employees collecting specimens in public places display proper identification.
Media reporting on disparities in COVID-19 test billing sparks renewed calls for increased transparency in medical laboratory test charges
Recent media reports of massive disparities in the prices charged for COVID-19 lab tests throughout the United States have citizens and law makers alike again calling for increased transparency in clinical laboratory test charges.
One recent example involves the New York Times (NYT), which after learning that Austin-based Gibson Diagnostic Labs (GDL) of Irving, Tex., billed a patient $2,315 for one COVID-19 test, questioned the disparity in coronavirus testing charges. The article, titled, “Most Coronavirus Tests Cost About $100. Why Did One Cost $2,315?” brought unwanted attention to the Texas clinical laboratory.
On July 16, the NYT reported that GDL, “has run some of the most expensive coronavirus tests in America.” In addition, the paper reported that health insurance companies have paid GDL $2,315 for individual COVID-19 tests, but that in “a couple of cases,” the price rose to $6,946. However, that higher amount resulted “when the lab said it mistakenly charged patients three times the base rate.”
In response to the NYT report, GDL released a statement that said, “In April 2020, a commercial insurer doing business with Gibson Diagnostic Labs inquired about the company’s pricing practices regarding COVID-19 testing. In response to the inquiry, the company conducted an internal review and identified commercial claims that were billed incorrectly by the company’s third-party biller. Because this incident did not meet our standards of quality, service, and compliance, the company terminated its relationship with the third-party biller.”
Gibson Diagnostic Labs (above) in Irving, Texas, recently drew the attention of the New York Times after, according to GDL, its third-party biller accidentally used an incorrect CPT code causing one COVID-19 test customer to receive a bill for $2,315. Further, the NYT reported that “[GDL] billed 117 tests at that price and had 23 of the claims paid in full. Some insurers paid partial reimbursements or sent back no money at all.” In a statement, GDL said it has corrected the mistake and reimbursed all affected parties. (Photo copyright: Dylan Hollingsworth/The New York Times.)
GDL Blames Third-party Biller for Errors
Responding to questions from Dark Daily, GDL provided details that were not previously reported. In an email, GDL said it worked closely with a NYT reporter by providing information about the incident, but that the reporter left out key information.
GDL also said that after the NYT’s inquiry, the lab reviewed its billing systems and learned that the CPT code for 23 COVID-19 commercial claims were transposed as a result of human error, resulting in payments totaling $53,255. The review also showed that the lab’s third-party biller had insufficient systems in place to prevent such errors.
“Upon learning this, we made the decision to terminate our contract with our third-party biller,” GDL said. “Finally, within 24-hours of identifying the billing error—and prior to the story being published—we rebilled all the claims, refunded payments to the respective payers, and followed up with each payer to ensure receipt of the corrected claims.
“Immediately after the claims were rebilled, we contacted all 205 patients who may have received an incorrect EOB [explanation of benefits], explained what happened, and apologized,” GDL stated.
Going forward, GDL said it will require its new biller to conduct regular audits each quarter and to maintain certain levels of automation and staffing to manage higher volume without disruption. GDL also said it regrets the disruption and inconvenience the billing error caused to its clients and patients.
Lessons for Clinical Laboratories
For clinical laboratories, there are at least four lessons that can be learned from GDL’s experience:
First, labs should be aware of how their own charges for all tests compare with what other labs charge, particularly when charging patients for high-profile tests, such as those for the new coronavirus. What Medicare and other payers charge for these tests has been reported widely, so that many patients are likely aware of the reasonable and customary charges for such tests.
Second, clinical labs may want to note that charging high prices for these tests could lead health insurers to increase their scrutiny of lab charges. The NYT article quoted Angela Meoli, a senior vice president at Aetna, saying, “We’ve seen a small number of laboratories that are charging egregious prices for COVID-19 tests.”
Third, coverage in the NYT often leads other publications to cover the same story. In this case, Kaiser Health News (KHN) and other news organizations have reported on what GDL charged and linked that story to their coverage of surprise medical bills.
Fourth, GDL recommends responding appropriately to journalists’ inquiries. However, lab should be aware that, even then, the news media may not report the facts as labs would prefer.
All of these lessons are important during the COVID-19 pandemic, because newspapers and other news organizations have encouraged consumers to submit copies of their lab tests and other bills. Such examples of charges above normal rates often generate unwanted coverage for hospitals, health systems, healthcare providers, and in this case, a clinical diagnostic laboratory.
All of this may be academic for those clinical laboratory managers and pathologists who scrupulously follow appropriate laws and guidelines for coding, billing, and collecting for clinical lab tests of all types—not just the COVID-19 test. But, year after year, there are individuals who operate certain clinical laboratories and who are willing to push their compliance with long-established laws and regulations for short-term profit. When these abusive lab practices surface and attract the attention of both federal prosecutors and national news media, it is the entire clinical laboratory profession that gets characterized in negative ways.
Certainly, many medical laboratory professionals would agree that the system of enforcing federal and state laws and pursuing obvious cases of fraudulent practices involving clinical lab testing leaves much to be desired. However, there are already several examples of federal prosecutors charging lab owners and managers for violating fraud and anti-kickback statutes in their marketing of COVID-19 tests. Hopefully the national news media will be effective in spotting illegal practices involving COVID-19 testing and bring more transparency to the lab testing marketplace.
Researchers found evidence indicating that the virus has—under selection pressure—made itself more stable, giving it a “significant boost in infectivity”
While the COVID-19 pandemic continues to spread across the United States and throughout the world, new research suggests that a coming genetic mutation within the SARS-CoV-2 coronavirus may make it much more dangerous than it already is. This finding has significant implications for clinical laboratories that perform COVID-19 testing and the in vitro diagnostics (IVD) companies that develop and manufacture tests for COVID-19.
The mutation, called D614G, will provide the coronavirus with sturdier spikes that will increase its ability to latch onto and infect cells. That’s according to a study conducted at The Scripps Research Institute (Scripps) in Jupiter, Fla., which found that a mutated coronavirus may be up to 10 times more infectious than the original strain.
“Viruses with this mutation were much more infectious than those without the mutation in the cell culture system we used,” said Hyeryun Choe, PhD, Professor, Department of Immunology and Microbiology, Scripps Research, and senior author of the study, in a Scripps news release.
A More Flexible and Potent Coronavirus May Be Coming
The researchers found that coronavirus particles containing the mutation tend to have four to five times more functional spikes than particles without the mutation. The spikes enable the virus to bind to cells more easily. The research suggests that the greater the number of functional spikes on the viral surface the greater the flexibility and potency of the coronavirus.
In the Scripps news release, Farzan said, “more flexible spikes allow newly made viral particles to navigate the journey from producer cell to target cell fully intact, with less tendency to fall apart prematurely.
“Over time, it has figured out how to hold on better and not fall apart until it needs to,” he added. “The virus has, under selection pressure, made itself more stable.”
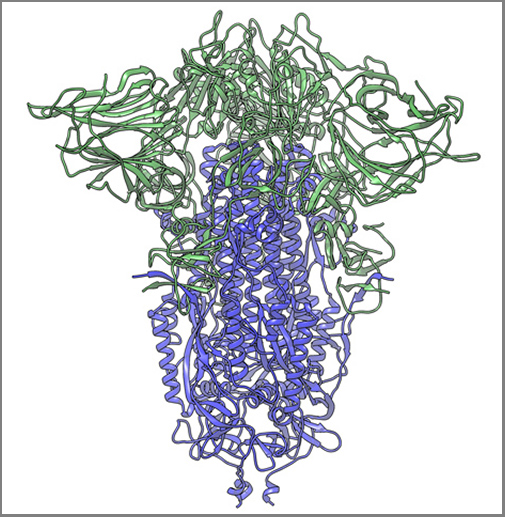
The image above, taken from the Scripps Research news release, shows “a cryogenic electron microscope image of a SARS-CoV-2 spike protein side view, the S1 section of the spike is shown in green and the S2 portion is shown in purple. This unique two-piece system has shown itself to be relatively unstable. A new mutation has appeared in the viral variant most common in New York and Italy that makes this spike both more stable and better able to infect cells.” (Graphic and caption copyright: Andrew Ward lab, Scripps Research.)
Mutation Makes SARS-CoV-2 Coronavirus ‘Much More Stable’
The two Scripps scientists have studied coronaviruses for nearly 20 years and performed extensive research on the Severe Acute Respiratory Syndrome (SARS) outbreak that occurred in 2003. They noted that there is a difference between spike proteins of SARS, an earlier strain of coronavirus, and the new SARS-CoV-2 strain.
The protein spikes of both strains were originally tripod shaped. However, the spikes of the SARS-CoV-2 coronavirus are divided into two different segments: S1 and S2. According to the published study: “The S1domain mediates receptor binding, and the S2 mediates downstream membrane fusion.”
This feature originally produced unstable spikes, but with the D614G mutation, the tripod breaks less frequently, which makes more of the spikes fully functional and the virus more infectious.
“Our data are very clear, the virus becomes much more stable with the mutation,” Choe said in the news release.
Is COVID-19 Spread Due to ‘Founder Effect’
The scientists also examined whether the spread of COVID-19 could have been the result of the “Founder Effect,” which is seen when a small number of variants fan out into a wide population by chance. Could the founder effect explain why COVID-19 outbreaks in some areas of the world were more severe than others? The researchers believe their data definitively answered that question.
“There have been at least a dozen scientific papers talking about the predominance of this mutation,” Farzan said. “Are we just seeing a founder effect? Our data nails it. It is not the founder effect.”
Hyeryun Choe, PhD (left), and Michael Farzan, PhD (right), scientists at Scripps Research explained that their research was performed using engineered viruses and that their observations of the virus and its mutation may not translate to increased transmissibility when a virus attaches to a host outside the lab. COVID-19 and its mutation appear to be relatively stable and are mutating at a rate slower than that of the seasonal flu, which may be critical factors in the development of a vaccine. (Photos copyright: Scripps Research.)
Findings Raise ‘Interesting’ Questions about the COVID-19 Coronavirus
Nevertheless, the two scientists are curious about some of their findings. “Our data raise interesting questions about the natural history of SARS-CoV-2 as it moved presumably from horseshoe bats to humans. At some point in this process, the virus acquired a furin-cleavage site, allowing its S1/S2 boundary to be cleaved in virus-producing cells. In contrast, the S1/S2 boundary of SARS-CoV-1, and indeed all SARS-like viruses isolated from bats, lack this polybasic site and are cleaved by TMPRSS2 or endosomalcathepsins in the target cells.
“In summary, we show that an S protein mutation that results in more transmissible SARS-CoV-2 also limits shedding of the S1 domain and increases S-protein incorporation into the virion. Further studies will be necessary to determine the impact of this change on the nature and severity of COVID-19,” the Scripps researchers concluded.
However, not all Scripps researchers agreed with the conclusions of Choe and Farzan’s research.
The Times of Israel reported that Kristian Andersen, PhD, a professor in the Department of Immunology and Microbiology, Scripps California Campus, told the New York Times that “other analyses of virus variants in labs had not found significant differences in infection rates.”
“That’s the main reason that I’m so hesitant at the moment,” Andersen said. “Because if one really was able to spread significantly better than the other, then we would expect to see a difference here, and we don’t.”
Times of Israel also reported that “In late May researchers in University College London said their studies of the genomes of more than 15,000 samples had not shown one strain being more infectious than others.”
So, the jury’s out. Nonetheless, clinical laboratory leaders will want to remain vigilant. A sudden increase in COVID-19 infection rates will put severe strain on already strained laboratory supply chains.
The CDC and US Navy study reveals common symptoms and suggests best protective measures to prevent spread in enclosed environments that clinical labs and pathology groups could use to protect their staff members
Results from a study conducted by the US Navy and the federal Centers for Disease Control and Prevention (CDC) of sailors onboard the USS Theodore Roosevelt during the recent COVID-19 outbreak aboard the ship may be useful for pathologists and clinical laboratory managers. The study also provides public health and infectious disease specialists with an opportunity to learn more about how the SARS-CoV-2 coronavirus spreads in enclosed environments.
The aircraft carrier garnered headlines in April due to a widespread outbreak of the coronavirus among its crew. The investigators asked crewmembers to complete a questionnaire and provide samples for a serological antibody test and molecular diagnostics test, reported the Navy’s Bureau of Medicine and Surgery (BUMED). The goal was to learn more about the disease and how it spreads in high-density environments. The COVID-19 tests were conducted April 20-24 while the ship was docked in Guam.
“This study paints a picture of current and prior SARS-CoV-2 infection among young adults living in close quarters,” said the study’s lead author Dan Payne, PhD, an epidemiologist at the CDC, in the BUMED statement. “This data will contribute to understanding COVID-19 in the US military, as well as among young adults in other close communal environments.”
Participation in the study was voluntary. At the time of testing, a total of 1,417 service members were still on the ship or at the base in Guam, the researchers wrote in their study. Among them, 383 crewmembers agreed to complete the survey and provide a blood sample for an enzyme-linked immunosorbent assay (ELISA) antibody test. Out of that group, 267 also provided nasal swab samples for a reverse transcription polymerase chain reaction (RT-PCR) molecular diagnostic test.
A clinical laboratory team from the Naval Hospital Guam and the Navy and Marine Corps Public Health Center are seen above collecting surveys, nasal swabs, and blood samples from sailors assigned to the aircraft carrier USS Theodore Roosevelt (CVN 71) during the investigation into the COVID-19 outbreak in April. The ship’s medical leaders established an emergency command center, initiated a roving and deep cleaning team, and continually educated the crew on social distancing and proper protective procedures and behaviors, to mitigate the spread of the SARS-CoV-2 coronavirus. (Photo copyright: US Navy.)
The questionnaire sought information about sailors’ demographic factors, health history, symptoms, and preventive behaviors, such as mask wearing and physical distancing. Crewmembers who tested positive for reactive antibodies received an additional test to detect presence of neutralizing antibodies that inhibit the virus.
The median age of participants was 30 years. About 75% were male. Only 28 (7.3%) reported comorbidities such as a history of asthma, diabetes, hypertension, or immunosuppression, which are considered risk factors for developing serious cases of the COVID-19 disease.
Key findings of the CDC/Navy’s study:
228 participants (59.7%) tested positive for reactive antibodies. Of those, 135 (59.2%) tested positive for neutralizing antibodies.
235 participants had previously tested positive in a SARS-CoV-2 diagnostic test. Of those, 212 (90.2%) tested positive for reactive antibodies.
A total of 238 participants had a previous or current SARS-CoV-2 infection. Of these, 18.5% reported no symptoms.
Of the 194 sailors who reported symptoms, 115 (59.3%) sought medical care, and two were hospitalized.
The most frequently reported symptoms were headache (66.5%), loss of taste or smell or both (61.3%); myalgia (56.2%); runny nose (55.7%); and fatigue (55.2%).
The most effective preventive measures were avoidance of common areas, increased physical distancing, and use of face coverings.
“What we saw was that most of the infections were actually mild, in addition to those that were asymptomatic,” Payne told reporters after the study was published, reported CNN. “And this is perhaps different from studies of older Americans, or maybe even those who were hospitalized already, and certainly much different from those with underlying health conditions.”
But with the high number of asymptomatic cases, “symptom-based surveillance might not detect all infections,” noted the researchers, who cautioned that “the analysis was conducted on a convenience sample of persons who might have had a higher likelihood of exposure, and all information was based on self-report, raising the possibility of selection and recall biases.”
In January, the crew of the Roosevelt totaled about 4,800 sailors, reported Defense One. However, after docking in Guam, many sailors were moved to hotel rooms for quarantine. As of May 5, at least 1,156 crewmembers had tested positive for infection, Stars and Stripes reported, and one had died.
Sailors aboard the USS Theodore Roosevelt were examined prior to reboarding the ship following off-ship quarantine or isolation. Only those found to be negative for the coronavirus, were allowed to board the ship. (Photo copyright: US Navy.)
Impact of COVID-19 on the USS Theodore Roosevelt’s Crew
As of April 6, 172 crew members had tested positive for COVID-19, including the ship’s captain Brett Crozier. At that time, 61% of the crew had received clinical laboratory testing and 1,999 sailors had been moved off the ship into quarantine, reported Defense One. By the next day, 270 sailors tested positive, a 57% increase from the previous day.
By April 14, 589 crew members were diagnosed positive for COVID-19. With 92% of the crew tested, 3,922 were found to be negative for the infection. Nevertheless, 4,024 sailors—nearly 83% of the crew—were moved into isolation quarters off-ship to prevent spread of the coronavirus.
In their study, the Navy/CDC researchers concluded: “In this convenience sample of young, healthy US service members experiencing close contact aboard an aircraft carrier, those with previous or current SARS-CoV-2 infection experienced mild illness overall, and nearly 20% were asymptomatic. Approximately one third of participants reported fever, myalgia, and chills and had higher odds of SARS-CoV-2 infection than did persons who reported cough and shortness of breath. Participants reporting anosmia (loss of sense of smell) or ageusia (loss of sense of taste) had 10 times the odds of having infection, compared with those who did not.
“In this sample of intensely exposed subjects, assessed at a single point in time, results demonstrated that antibodies developed and that, at the time of specimen collection, many of these were neutralizing antibodies. … This is a promising indicator of immunity, and in several participants, neutralizing antibodies were still detectable >40 days after symptom onset. Ongoing studies assessing the humoral antibody response over time will aid the interpretation of serologic results in an outbreak investigation such as this.
“These results provide new indications of symptomatology of SARS-CoV-2 infections and serologic responses among a cohort of young US adults living in a congregate environment and contribute to a better understanding of COVID-19 epidemiology in the US military. The findings reinforce the importance of nonpharmaceutical interventions such as wearing a face covering, avoiding common areas, and observing social distancing to lower risk for infection in similar congregate living settings.”
Not all the specific lessons learned from this COVID-19 outbreak aboard a US Navy vessel will be applicable to clinical laboratories and anatomic pathology groups. Nevertheless, it is probable that the data gleaned from the CDC/Navy study aboard the USS Theodore Roosevelt will someday mean civilian Americans can count on improved responses to disease outbreaks from the nation’s testing laboratories.
Charges against this life science company executive include healthcare fraud as well as the first COVID-19 related securities fraud
In the first securities fraud prosecution involving clinical laboratory COVID-19 testing, the US federal Department of Justice (DOJ) charged the president of a Sunnyvale, Calif., life sciences biotechnology company with participating in a scheme to mislead investors and also to commit healthcare fraud, stated a DOJ press release.
The DOJ charged Mark Schena, PhD, president of Arrayit Corporation, with one count of securities fraud and one count of conspiracy to commit healthcare fraud related to submissions of more than $69 million in claims for allegedly unnecessary medical laboratory allergy and COVID-19 tests, the Associated Press (AP) reported.
“The defendant allegedly defrauded Medicare through illegal kickbacks and bribes, and then turned to exploiting the pandemic by fraudulently promoting an unproven COVID-19 test to the market,” said Brian Benczkowski, DOJ Assistant Attorney General, Criminal Division, in the DOJ press release.
According to the Washington Post, Arrayit allegedly bundled its finger-stick allergy test with the COVID-19 test kit.
Authorities Question Bundling of Tests, Claims
An affidavit in support of the criminal complaint stated that Arrayit was promoting “‘microarray technology’ for allergy and COVID-19 testing that allows for laboratory testing on a finger prick drop of blood that is placed on a paper card and sent by mail to Arrayit’s laboratory.”
The government’s investigation actually goes back two years to a time when Arrayit allegedly submitted or caused submission of $5.9 million in Medicare lab test claims and $63 million in lab test claims to private insurers through bribes and kickbacks, MedTech Dive reported.
The company’s clinical laboratory test for COVID-19 failed to receive US Food and Drug Administration Emergency Use Authorization (EUA), because it did not have the level of specificity and sensitivity required, MedTech Dive noted.
“Schena offered an Arrayit COVID-19 test in order to obtain Medicare beneficiary information that then was used to submit false and fraudulent claims for an unrelated and far more expensive allergy test for 120 allergens,” the DOJ complaint stated, adding, “Schena and others transmitted false and fraudulent e-mail communications and marketing materials about the Arrayit COVID-19 test and purported need to bundle the COVID-19 test with Arrayit’s allergy test, while never disclosing there were substantial questions about the accuracy of Arrayit’s COVID-19 test.”
Highlights of DOJ Charges
According to the DOJ press release:
Schena and others from 2018 through February allegedly “paid kickbacks and bribes” to recruiters and doctors to run a medical laboratory test for allergy screening (with 120 allergens) on patients “regardless of medical necessity and then make numerous misrepresentations to potential investors.”
News releases and social media promoted partnerships with companies and government agencies that either “did not exist” or were minor.
As the pandemic heated up, Arrayit representatives “made false claims concerning Arrayit’s ability to provide accurate, fast, reliable and cheap COVID-19 tests in compliance with state and federal regulations,” prosecutors said.
According to the DOJ’s complaint, Schena told investigators developing a test for COVID-19 was “like a pastry chef” who switches from selling “strawberry pies” to selling “rhubarb and strawberry pies.”
“The allure of cheap reliable alternatives to today’s standard blood tests panels has captured the imagination of the healthcare industry, making such alternatives a prime subject for fraudsters,” said David Anderson (above), US Attorney for the Northern District of California, in the DOJ press release, adding, “The scheme described in the complaint, in which the defendant allegedly leveraged this allure by appending the fear of the COVID-19 pandemic, amounts to a cynical multi-million-dollar hoax.” (Photo copyright: San Francisco Examiner.)
DOJ Prioritizing Coronavirus Fraud
US Attorney General William Barr earlier this year called for prioritization of investigation and prosecution of coronavirus fraud schemes, noted a DOJ statement, which pointed out that these types of fraud schemes leverage COVID-19 testing information generated by healthcare providers to fraudulently bill Medicare for other tests and procedures.
In April, Dark Daily’s sister publication, The Dark Report (TDR), covered one such kickback scheme in Georgia the DOJ was investigating. In that case, a Georgia man allegedly participated in a fraudulent kickback scheme in which clinical laboratory companies paid him on a per-test basis for referring cancer genetic, coronavirus, and respiratory pathogen panel tests to labs, TDR noted.
Clearly, the DOJ is stepping up its investigation into COVID-19 test fraud. Thus, medical laboratory leaders and pathologists should remain vigilant, as they are likely to observe more enforcement activity as the pandemic persists.