Clinical laboratories and pathology groups can benefit from knowing how genetic testing is being used for other than medical testing purposes
It is useful for pathologists and clinical laboratory managers to be aware of the different ways genetic testing and DNA sequencing is being conducted. That’s because a genetic test for one purpose—such as identifying an individual’s relatives and connection to a region or a cultural group—might generate data that could become part of that person’s medical care.
Thus, an ongoing genetic study in South Africa highlighting the issue of so-called “helicopter research” will be informative for Dark Daily’s readers.
Also known as “neo-colonial science,” helicopter research describes when scientists from wealthy countries perform research in lower-income countries in ways that may be deemed exploitative or disrespectful to local populations.
“Scientists conduct helicopter research when they collect data from developing countries and marginalized communities with little to no involvement from local researchers and community members,” wrote researchers Dana Al-Hindi, and Brenna Henn PhD, in an article for The Conversation. “Helicopter research also occurs when researchers take data out of the country they collected it from without either providing benefit to or sharing the results with the community.”
In an article for The Conversation, UC Davis researchers Brenna Henn, PhD (left), and Dana Al-Hindi (right), wrote, “While we have learned a great deal from these communities, we have been unable to fulfill a common request: providing them their individual genetic ancestry result. In our attempts to overcome the logistical challenges of providing this information, we’ve grappled with the common question of how to ensure an equitable balance of benefits between researchers and the community they study. What we’ve found is that there is no easy answer.” Clinical laboratories will want to remember the term “Helicopter Research” in relation to these types of studies. (Photos copyright: UC Davis/The Conversation.)
The South Africa study, conducted over the past 12 years, aims to use genetic data “to help unravel the history and prehistory of southern Africans and their relationship to populations around the world,” the authors wrote in The Conversation.
The researchers have been using the genetic data to trace the ancestry of indigenous Khoekhoe and San peoples in South Africa as well as other populations that self-identify as “Colored.”
“Early European colonizers initially used this term to refer to indigenous Khoekhoe and San groups long before it was codified by the apartheid government in 1948,” the researchers wrote. “It persists today as an ethnic category, broadly encompassing Khoe-San groups, various East African, Indian, and Southeast Asian populations brought by the slave trade, and people of mixed ancestry.”
Challenges Sharing Genetic Data with Study Participants
Participants in the study have asked to see their personal genetic ancestry results, but the researchers noted several challenges, including local restrictions and the difficulty of presenting complex data in “an accessible and digestible form.” So, the researchers partnered with consumer-focused genetic testing company 23andMe (NASDAQ:ME).
23andMe provided additional funding for the research, assisted the researchers in community outreach, and “expanded our ability to ‘capacity-build’—that is, to make sure that the knowledge and skills we gain are shared with local institutions,” Henn and Al-Hindi wrote in The Conversation. They added that they are still dealing with questions about whether their efforts to provide equitable benefits are sufficient.
“Our research team, local collaborators, and 23andMe are all concerned about how to best address the risk of helicopter research, coercion, and any unknown risks that may arise from disclosing personal ancestry results,” they wrote.
Cape Town Statement on Fostering Research Integrity
The issue of helicopter research was a major focus at the 7th World Conference on Research Integrity (WCRI), held May 29-June 1 in Cape Town, South Africa. It was the first WCRI to be held in Africa and adopted the theme “Fostering Research Integrity in an Unequal World.”
One outcome of the conference will be an effort to produce what is known as the Cape Town Statement on Fostering Research Integrity. The statement will “highlight the importance of fairness in international research partnerships,” noted Research Professional News.
The statement “compels institutions and researchers alike to act on their responsibilities to promote equity, diversity, and fairness in research partnerships,” conference speaker Retha Visagie, DCur, told the publication. She leads the Research Integrity Office at the University of South Africa.
Conference co-chair Lyn Horn, PhD, director the Office of Research Integrity at the University of Cape Town, told the publication that it could take up to a year before a draft of the statement is ready for comment.
One overarching goal will be to “demonstrate why inequity and unfair practices in research collaborations and contexts is a research integrity (RI) matter,” the authors wrote. “Second it must identify some key values or principles and action guides that will address the issue of equity and fairness in research within the context of the complete research life cycle from research agenda setting and call to proposal development, through grant application, allocation and management of funding, data production, analysis, management and sharing, to outputs, translation, and evaluation.”
Another conference speaker, Francis Kombe PhD, told attendees the statement will offer guidance specifically to institutions such as universities, journals, and funding organizations, the journal Science reported. That stands in contrast to earlier statements on helicopter research, which were geared more toward individuals and small groups.
How any of this will impact clinical laboratories and pathology groups remains unclear. Nevertheless, it is worthwhile knowing how gene sequencing is being used by researchers for purposes other than to guide diagnoses and treatment of patients.
Researchers find declining antibody levels in SARS-CoV-2 patients are offset by T cells and B cells that remain behind to fight off reinfection
Questions remain regarding how long antibodies produced by a COVID-19 vaccine or natural infection will provide ongoing protection against SARS-CoV-2. However, a new study showing COVID-19 immunity may be “robust” and “long lasting” may signal important news for clinical laboratories and in vitro diagnostics companies developing serological tests for the coronavirus disease.
The LJI research team analyzed blood samples from 188 COVID-19 patients, 7% of whom had been hospitalized. They measured not only virus-specific antibodies in the blood stream, but also memory B cell infections, T helper cells, and cytotoxic (killer) T cells.
While antibodies eventually disappear from the blood stream, T cells and B cells appear to remain to fight future reinfection.
“As far as we know, this is the largest study ever for any acute infection that has measured all four of those components of immune memory,” Crotty said in a La Jolla Institute news release.
The LJI researchers found that virus-specific antibodies remained in the blood stream months after infection while spike-specific memory B cells—which could trigger an accelerated and robust antibody-mediated immune response in the event of reinfection—actually increased in the body after six months. In addition, COVID-19 survivors had an army of T cells ready to halt reinfection.
“Our data show immune memory in at least three immunological compartments was measurable in ~95% of subjects five to eight months post symptom onset, indicating that durable immunity against secondary COVID-19 disease is a possibility in most individuals,” the study concludes. The small percentage of the population found not to have long-lasting immunity following COVID-19 infection could be vaccinated in an effort to stop reinfection from occurring on the way to achieving herd immunity, the LJI researchers maintained.
Do COVID-19 Vaccines Create Equal Immunity Against Reinfection?
Whether COVID-19 vaccinations will provide the same immune response as an active infection has yet to be determined, but indications are protection may be equally strong.
“It is possible that immune memory will be similarly long lasting similar following vaccination, but we will have to wait until the data come in to be able to tell for sure,”
LJI Research Professor Daniela Weiskopf, PhD, said in the LJI statement. “Several months ago, our studies showed that natural infection induced a strong response, and this study now shows that the response lasts. The vaccine studies are at the initial stages, and so far, have been associated with strong protection. We are hopeful that a similar pattern of responses lasting over time will also emerge for the vaccine-induced responses.”
The study’s authors cautioned that people previously diagnosed with COVID-19 should not assume they have protective immunity from reinfection, the Washington Post noted. In fact, according to the LJI news release, researchers saw a “100-fold range in the magnitude of immune memory.”
Alessandro Sette, Doctor of Biological Sciences (above), an Italian immunologist, Professor at the Center for Autoimmunity and Inflammation/Center for Infectious Disease and Vaccine Research at La Jolla Institute for Immunology, and co-author of the study, told the Washington Post that people should act responsibly. “If I had COVID, I would still not throw away my masks, I would not go to rave parties … It’s like driving a car where you know you have 90% probability that the brakes work.” (Photo copyright: La Jolla Institute for Immunology.)
Previous Studies Found Little Natural Immunity Against SARS-CoV-2 Reinfection
The Scientist reported that several widely publicized previous studies raised concerns that immunity from natural infection was fleeting, perhaps dwindling in weeks or months. And a United Kingdom study published in Nature Microbiology found that COVID-19 generated “only a transient neutralizing antibody response that rapidly wanes” in patients who exhibited milder infection.
Daniel M. Davis, PhD, Professor of Immunology at the University of Manchester, says more research is needed before scientists can know for certain how long COVID-19 immunity lasts after natural infection.
“Overall, these results are interesting and provocative, but more research is needed, following large numbers of people over time. Only then, will we clearly know how many people produce antibodies when infected with coronavirus, and for how long,” Davis told Newsweek.
While additional peer-reviewed studies on the body’s immune response to COVID-19 will be needed, this latest study from the La Jolla Institute for Immunity may help guide clinical laboratories and in vitro diagnostic companies that are developing serological antibody tests for COVID-19 and lead to more definitive answers as to how long antibodies confer protective immunity.
The St. Louis-based in vitro diagnostics (IVD) developer is making PrecivityAD available to physicians while awaiting FDA clearance for the non-invasive test
Clinical laboratories have long awaited a test for Alzheimer’s disease and the wait may soon be over. The first blood test to aid physicians and clinical laboratories in the diagnosis of patients with memory and cognitive issues has been released by C₂N Diagnostics of St. Louis. The test measures biomarkers associated with amyloid plaques in the brain—the pathological hallmark of Alzheimer’s.
In a news release, PrecivityAD describes the laboratory-developed test (LDT) as “a highly sensitive blood test using mass spectrometry and is performed in C₂N’s CLIA-certified laboratory. While the test by itself cannot diagnose Alzheimer’s disease … the test is an important new tool for physicians to aid in the evaluation process.”
PrecivityAD provides physicians with an Amyloid Probability Score (APS) for each patient. For example:
A low APS (0-36) is consistent with a negative amyloid PET scan result and, thus, has a low likelihood of amyloid plaques, an indication other causes of cognitive symptoms should be investigated.
An intermediate APS (37-57) does not distinguish between the presence or absence of amyloid plaques and indicates further diagnostic evaluation may be needed to assess the underlying cause(s) for the patient’s cognitive symptoms.
A high APS (58-100) is consistent with a positive amyloid positron-emission tomography (PET) scan result and, thus, a high likelihood of amyloid plaques. Presence of amyloid plaques is consistent with an Alzheimer’s disease diagnosis in someone who has cognitive decline, but alone is insufficient for a final diagnosis.
The $1,250 test is not currently covered by health insurance or Medicare. However, C₂N Diagnostics has pledged to offer discounts to patients based on income levels.
Jeff Cummings, MD, ScD (above) Research Professor, Department of Brain Health, University of Nevada, Las Vegas, said in a C₂N Diagnostics press release, “A blood test for Alzheimer’s is a game changer.” While there is no cure for Alzheimer’s, a non-invasive blood test can help providers diagnose patients when their symptoms are mild and often misdiagnosed. “Advances in Alzheimer’s diagnostics are key to more effective identification, diagnosis, and clinical trial recruitment,” he added. Currently, brain changes caused by the disease are most commonly identified through PET scans. (Photo copyright: University of Nevada Las Vegas.)
Additional Research Requested
While C₂N’s PrecivityAD is the first test of its kind to reach the commercial market, it has not received US Food and Drug Administration (FDA) clearance, nor has the company published detailed data on the test’s accuracy. However, the PrecivityAD website says the laboratory-developed test “correctly identified brain amyloid plaque status (as determined by quantitative PET scans) in 86%” of 686 patients, all of whom were older than 60 years of age with subjective cognitive impairment or dementia.
But some Alzheimer’s advocacy groups are tempering their enthusiasm about the breakthrough. Eliezer Masliah, MD, Director of the Division of Neuroscience, National Institute on Aging, told the Associated Press (AP), “I would be cautious about interpreting any of these things,” he said of the company’s claims. “We’re encouraged, we’re interested, we’re funding this work, but we want to see results.”
Heather Snyder, PhD, Vice President, Medical and Scientific Relations at the Alzheimer’s Association told the AP her organization will not endorse a test without FDA clearance. The Alzheimer’s Association also would like to see the test studied in larger and diverse populations. “It’s not quite clear how accurate or generalizable the results are,” she said.
Braunstein defended the decision to make the test for Alzheimer’s immediately available to physicians, asking in the AP article, “Should we be holding that technology back when it could have a big impact on patient care?”
Howard Fillit, MD, Founding Executive Director and Chief Science Officer of the Alzheimer’s Drug Discovery Foundation (ADDF), maintains the first-of-its-kind blood test is an important milestone in Alzheimer’s research. ADDF invested in C₂N’s development of the test.
“Investing in biomarker research has been a core goal for the ADDF because having reliable, accessible, and affordable biomarkers for Alzheimer’s diagnosis is step one in finding drugs to prevent, slow, and even cure the disease,” Fillit said in an ADDF news release.
C₂N is also developing a Brain Health Panel to detect multiple blood-based markers for Alzheimer’s disease that will aid in better disease staging, treatment monitoring, and differential diagnosis.
Second Alzheimer’s Test in Development
Soon medical laboratories may have two different in vitro diagnostic tests for Alzheimer’s disease. On December 2, Fujirebio Diagnostics filed for FDA 510(k) premarket clearance for its Lumipulse G β-Amyloid Ratio (1-42/1-40) test, which looks for biomarkers found in cerebral spinal fluid.
“Accurate and earlier intervention will also facilitate the development of new drug therapies, which are urgently needed as the prevalence of Alzheimer’s disease increases with a rapidly aging population globally,” Fujirebio Diagnostics President and CEO Monte Wiltse said in a news release.
The Lumipulse G β-Amyloid test, which is intended for use in patients aged 50 and over presenting with cognitive impairment, has received CE-marking for use in the European Union.
Clinical laboratory managers will want to keep a close eye on rapidly evolving developments in testing for Alzheimer’s disease. It is the sixth leading cause of death in the United States and any clinical laboratory test that could produce an early and accurate diagnosis of Alzheimer’s Disease would become a valuable tool for physicians who treat patients with the symptoms of Alzheimer’s.
The AI protein-structure-prediction system may ‘revolutionize life sciences by enabling researchers to better understand disease,’ researchers say
Genomics leaders watched with enthusiasm as artificial intelligence (AI) accelerated discoveries that led to new clinical laboratory diagnostic tests and advanced the evolution of personalized medicine. Now Google’s London-based DeepMind has taken that a quantum step further by demonstrating its AI can predict the shape of proteins to within the width of one atom and model three-dimensional (3D) structures of proteins that scientist have been trying to map accurately for 50 years.
Pathologists and clinical laboratory professionals know that it is estimated that there are around 30,000 human genes. But the human proteome has a much larger number of unique proteins. The total number is still uncertain because scientists continue to identify new human proteins. For this reason, more knowledge of the human protein is expected to trigger an expanding number of new assays that can be used by medical laboratories for diagnostic, therapeutic, and patient-monitoring purposes.
DeepMind’s AI tool is called AlphaFold and the protein-structure-prediction system will enable scientists to quickly move from knowing a protein’s DNA sequence to determining its 3D shape without time-consuming experimentation. It “is expected to accelerate research into a host of illnesses, including COVID-19,” BBC News reported.
This protein-folding breakthrough not only answers one of biology’s biggest mysteries, but also has the potential to revolutionize life sciences by enabling researchers to better understand disease processes and design personalized therapies that target specific proteins.
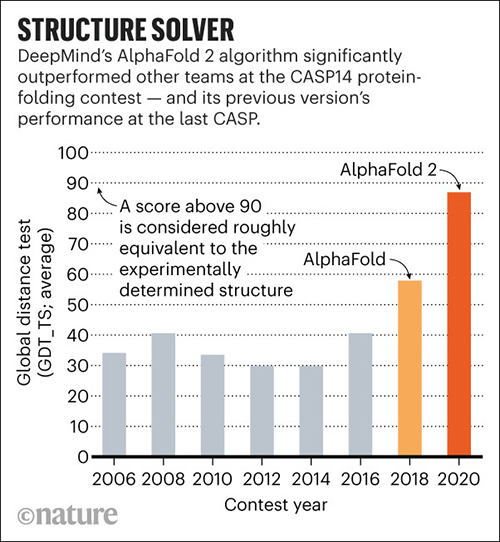
In November, DeepMind’s AlphaFold won the 14th Community Wide Experiment on Critical Assessment of Techniques for Protein Structure Prediction (CASP14), a biennial competition in which entrants receive amino acid sequences for about 100 proteins whose 3D structures are unknown. By comparing the computational predictions with the lab results, each CASP14 competitor received a global distance test (GDT) score. Scores above 90 out of 100 are considered equal to experimental methods. AlphaFold produced models for about two-thirds of the CASP14 target proteins with GDT scores above 90, a CASP14 press release states.
According to MIT Technology Review, DeepMind’s discovery is significant. That’s because its speed at predicting the structure of proteins is unprecedented and it matched the accuracy of several techniques used in clinical laboratories, including:
Unlike the laboratory techniques, which, MIT noted, are “expensive and slow” and “can take hundreds of thousands of dollars and years of trial and error for each protein,” AlphaFold can predict a protein’s shape in a few days.
“AlphaFold is a once in a generation advance, predicting protein structures with incredible speed and precision,” Arthur D. Levinson, PhD, Founder and CEO of Calico Life Sciences, said in a DeepMind blogpost. “This leap forward demonstrates how computational methods are poised to transform research in biology and hold much promise for accelerating the drug discovery process.”
Science reported that AlphaFold, which scored a median of 87—25 points above the next best predictions—did so well that CASP14 organizers worried DeepMind may have been somehow cheated. To validate the results, they asked AlphaFold to complete a “special challenge”—modeling a membrane protein from an ancient species of microbes called archaea, which they had been unable to model satisfactorily using X-ray crystallography. AlphaFold returned a detailed image of a three-part protein with two long helical arms in the middle. “It’s almost perfect,” Andrei Lupas, PhD, Director at the Max Planck Institute for Developmental Biology, told Science. “They could not possibly have cheated on this. I don’t know how they do it.” (Graphic copyright: DeepMind/Nature.)
“Even tiny rearrangements of these vital molecules can have catastrophic effects on our health, so one of the most efficient ways to understand disease and find new treatments is to study the proteins involved,” Moult said in the CASP14 press release. “There are tens of thousands of human proteins and many billions in other species, including bacteria and viruses, but working out the shape of just one requires expensive equipment and can take years.”
Science reported that the 3D structures of only 170,000 proteins have been solved, leaving roughly 200 million proteins that have yet to be modeled. Therefore, AlphaFold will help researchers in the fields of genomics, microbiomics, proteomics, and other omics understand the structure of protein complexes.
“Being able to investigate the shape of proteins quickly and accurately has the potential to revolutionize life sciences,” Andriy Kryshtafovych, PhD, Project Scientist at University of California, Davis, Genome Center, said in the press release. “Now that the problem has been largely solved for single proteins, the way is open for development of new methods for determining the shape of protein complexes—collections of proteins that work together to form much of the machinery of life, and for other applications.”
Clinical laboratories play a major role in the study of human biology. This breakthrough in genomics research and new insights into proteomics may provide opportunities for medical labs to develop new diagnostic tools and assays that better identify proteins of interest for diagnostic and therapeutic purposes.
Scientist described the speed at which SARS-CoV-2’s full sequence of genetic material was made public as ‘unprecedented’ and medical labs are rushing to validate tests for this new disease
In the United States, headlines scream about the lack of
testing for the novel Coronavirus
disease 2019 (COVID-19). News reporters ask daily why it is taking so long
for the US healthcare system to begin testing large numbers of patients for
SARS-CoV-2, the virus that causes COVID-19. Yet, pathologists
and clinical
laboratory scientists know that new technologies for gene sequencing
and diagnostic testing are helping public health laboratories bring up tests
for a previously unknown new disease faster than at any time in the past.
At the center of the effort to develop accurate new assays
to detect SARS-CoV-2 and help diagnose cases of the COVID-19 disease are medical laboratory
scientists working in public health
laboratories, in academic medical centers, and in research labs across the
United States. Their collective efforts are producing results on a faster
timeline than in any previous discovery of a new infectious disease.
For example, during the severe
acute respiratory syndrome (SARS) outbreak in 2003, five months passed
between the first recognized case of the disease in China and when a team of
Canadian scientists cracked the genetic code of the virus, which was needed to
definitively diagnose SARS patients, ABC
News reported.
In contrast, Chinese scientists sequenced this year’s
coronavirus (originally named 2019-nCoV) and made it available on Jan. 10,
2020, just weeks after public health officials in Wuhan, China, reported the
first case of pneumonia from the unknown virus to the World Health Organization
(WHO), STAT
reported.
Increases in sequencing speed enabled biotechnology
companies to quickly create synthetic copies of the virus needed for research. Roughly
two weeks later, scientists completed sequencing nearly two dozen more samples
from different patients diagnosed with COVID-19.
Molecular biologist Kristian Andersen, PhD (above right, with graduate students who helped sequence the Zika virus), an Associate Professor in the Department of Immunology and Microbiology at Scripps Research in California and Director of Infectious Disease Genomics at Scripps’ Translational Research Institute, worked on the team that sequenced the Ebola genome during the 2014 outbreak. He told STAT that the pace of sequencing of the SARS-CoV-2 coronavirus is “unprecedented.” (Photo copyright: Scripps Research.)
Lower Sequencing Costs Speed COVID-19 Diagnostics Research
Additionally, a significant decline in the cost of genetic synthesis is playing an equally important role in helping scientists slow the spread of COVID-19.In its coverage of the SARS-CoV-2 outbreak, The Verge noted that two decades ago “it cost $10 to create a synthetic copy of one single nucleotide, the building block of genetic material. Now, it’s under 10 cents.” Since the coronavirus gene is about 30,000 nucleotides long, that price reduction is significant.
Faster sequencing and cheaper access to synthetic copies is
contributing to the development of diagnostic tests for COVID-19, an important
step in slowing the disease.
“This continues to be an evolving situation and the ability to distribute this diagnostic test to qualified medical laboratories is a critical step forward in protecting the public health,” FDA Commissioner Stephen M. Hahn, MD, said in an FDA statement.
However, the Washington Post soon reported that the government-created coronavirus test kits contained a “faulty component,” which as of February 25 had limited testing in the US to only 426 people, not including passengers who returned to the US on evacuation flights. The Post noted that the nation’s public health laboratories took “the unusual step of appealing to the FDA for permission to develop and use their own [laboratory-developed] tests” for the coronavirus.
“This is an extraordinary request, but this is an extraordinary time,” Scott Becker,
Parallel efforts to develop and validate tests for COVID-19
are happening at the clinical laboratories of academic medical centers and in a
number of commercial laboratory companies. As these labs show their tests meet
FDA criteria, they become available for use by physicians and other healthcare
providers.
Dark Daily’s sister publication, The Dark Report just published an intelligence briefing about the urgent effort at the clinical laboratory of Northwell Health to develop both a manual COVID-19 assay and a test that can be run on the automated analyzers already in use in the labs at Northwell Health’s 23 hospitals. (See TDR, “Northwell Lab Team Validates COVID-19 Test on Fast Timeline,” March 9, 2020.)
Following the FDA’s March 13 EUA for the Thermo Fisher test,
Hahn said, “We have been engaging with test developers and encouraging them to
come to the FDA and work with us. Since the beginning of this outbreak, more
than 80 test developers have sought our assistance with development and
validation of tests they plan to bring through the Emergency Use Authorization
process. Additionally,” he continued, “more than 30 laboratories have notified
us they are testing or intend to begin testing soon under our new policy for
laboratory-developed tests for this emergency. The number of products in the
pipeline reflects the significant role diagnostics play in this outbreak and
the large number of organizations we are working with to bring tests to
market.”
Pharma Company Uses Sequencing Data to Develop Vaccine in
Record Time
Even as clinical laboratories work to develop and validate diagnostic tests for COVID-19, drug manufacturers are moving rapidly to develop a COVID-19 vaccine. In February, Massachusetts-based biotechnology company Moderna Therapeutics (NASDAQ:MRNA) announced it had shipped the first vials of its potential coronavirus vaccine (mRNA-1273) to the National Institute of Allergy and Infectious Disease (NIAID) for use in a Phase One clinical trial.
“The collaboration across Moderna, with NIAID, and with CEPI [Coalition for Epidemic Preparedness Innovations] has allowed us to deliver a clinical batch in 42 days from sequence identification,” Juan Andres, Chief Technical Operations and Quality Officer at Moderna, stated in a news release.
The Wall Street Journal (WSJ) reported that NIAID expects to start a clinical trial of about 20 to 25 healthy volunteers by the end of April, with results available as early as July or August.
“Going into a Phase One trial within three months of getting the sequence is unquestionably the world indoor record,” NIAID Director Anthony Fauci, MD, told the WSJ. “Nothing has ever gone that fast.”
There are no guarantees that Moderna’s coronavirus vaccine
will work. Furthermore, it will require further studies and regulatory
clearances that could delay widespread distribution until next year.
Nonetheless, Fauci told the WSJ, “The only way you
can completely suppress an emerging infectious disease is with a vaccine. If
you want to really get it quickly, you’re using technologies that are not as
time-honored as the standard, what I call antiquated, way of doing it.”
In many ways, the news media has overlooked all the important
differences in how fast useful diagnostic and therapeutic solutions for
COVID-19 are moving from research settings into clinical use, when compared to
early episodes of the emergence of a new infectious disease, such as SARS in
2003.
The story the American public has yet to learn is how new
genetic sequencing technologies, improved diagnostic methods, and enhanced
informatics capabilities are being used by researchers, pathologists, and
clinical laboratory professionals to understand this new disease and give
healthcare professionals the tools they need to diagnose, treat, and monitor
patients with COVID-19.