Researchers found evidence indicating that the virus has—under selection pressure—made itself more stable, giving it a “significant boost in infectivity”
While the COVID-19 pandemic continues to spread across the United States and throughout the world, new research suggests that a coming genetic mutation within the SARS-CoV-2 coronavirus may make it much more dangerous than it already is. This finding has significant implications for clinical laboratories that perform COVID-19 testing and the in vitro diagnostics (IVD) companies that develop and manufacture tests for COVID-19.
The mutation, called D614G, will provide the coronavirus with sturdier spikes that will increase its ability to latch onto and infect cells. That’s according to a study conducted at The Scripps Research Institute (Scripps) in Jupiter, Fla., which found that a mutated coronavirus may be up to 10 times more infectious than the original strain.
“Viruses with this mutation were much more infectious than those without the mutation in the cell culture system we used,” said Hyeryun Choe, PhD, Professor, Department of Immunology and Microbiology, Scripps Research, and senior author of the study, in a Scripps news release.
A More Flexible and Potent Coronavirus May Be Coming
The researchers found that coronavirus particles containing the mutation tend to have four to five times more functional spikes than particles without the mutation. The spikes enable the virus to bind to cells more easily. The research suggests that the greater the number of functional spikes on the viral surface the greater the flexibility and potency of the coronavirus.
In the Scripps news release, Farzan said, “more flexible spikes allow newly made viral particles to navigate the journey from producer cell to target cell fully intact, with less tendency to fall apart prematurely.
“Over time, it has figured out how to hold on better and not fall apart until it needs to,” he added. “The virus has, under selection pressure, made itself more stable.”
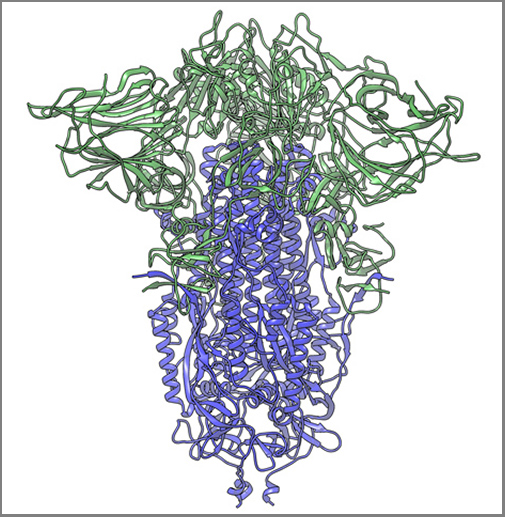
The image above, taken from the Scripps Research news release, shows “a cryogenic electron microscope image of a SARS-CoV-2 spike protein side view, the S1 section of the spike is shown in green and the S2 portion is shown in purple. This unique two-piece system has shown itself to be relatively unstable. A new mutation has appeared in the viral variant most common in New York and Italy that makes this spike both more stable and better able to infect cells.” (Graphic and caption copyright: Andrew Ward lab, Scripps Research.)
Mutation Makes SARS-CoV-2 Coronavirus ‘Much More Stable’
The two Scripps scientists have studied coronaviruses for nearly 20 years and performed extensive research on the Severe Acute Respiratory Syndrome (SARS) outbreak that occurred in 2003. They noted that there is a difference between spike proteins of SARS, an earlier strain of coronavirus, and the new SARS-CoV-2 strain.
The protein spikes of both strains were originally tripod shaped. However, the spikes of the SARS-CoV-2 coronavirus are divided into two different segments: S1 and S2. According to the published study: “The S1domain mediates receptor binding, and the S2 mediates downstream membrane fusion.”
This feature originally produced unstable spikes, but with the D614G mutation, the tripod breaks less frequently, which makes more of the spikes fully functional and the virus more infectious.
“Our data are very clear, the virus becomes much more stable with the mutation,” Choe said in the news release.
Is COVID-19 Spread Due to ‘Founder Effect’
The scientists also examined whether the spread of COVID-19 could have been the result of the “Founder Effect,” which is seen when a small number of variants fan out into a wide population by chance. Could the founder effect explain why COVID-19 outbreaks in some areas of the world were more severe than others? The researchers believe their data definitively answered that question.
“There have been at least a dozen scientific papers talking about the predominance of this mutation,” Farzan said. “Are we just seeing a founder effect? Our data nails it. It is not the founder effect.”
Hyeryun Choe, PhD (left), and Michael Farzan, PhD (right), scientists at Scripps Research explained that their research was performed using engineered viruses and that their observations of the virus and its mutation may not translate to increased transmissibility when a virus attaches to a host outside the lab. COVID-19 and its mutation appear to be relatively stable and are mutating at a rate slower than that of the seasonal flu, which may be critical factors in the development of a vaccine. (Photos copyright: Scripps Research.)
Findings Raise ‘Interesting’ Questions about the COVID-19 Coronavirus
Nevertheless, the two scientists are curious about some of their findings. “Our data raise interesting questions about the natural history of SARS-CoV-2 as it moved presumably from horseshoe bats to humans. At some point in this process, the virus acquired a furin-cleavage site, allowing its S1/S2 boundary to be cleaved in virus-producing cells. In contrast, the S1/S2 boundary of SARS-CoV-1, and indeed all SARS-like viruses isolated from bats, lack this polybasic site and are cleaved by TMPRSS2 or endosomalcathepsins in the target cells.
“In summary, we show that an S protein mutation that results in more transmissible SARS-CoV-2 also limits shedding of the S1 domain and increases S-protein incorporation into the virion. Further studies will be necessary to determine the impact of this change on the nature and severity of COVID-19,” the Scripps researchers concluded.
However, not all Scripps researchers agreed with the conclusions of Choe and Farzan’s research.
The Times of Israel reported that Kristian Andersen, PhD, a professor in the Department of Immunology and Microbiology, Scripps California Campus, told the New York Times that “other analyses of virus variants in labs had not found significant differences in infection rates.”
“That’s the main reason that I’m so hesitant at the moment,” Andersen said. “Because if one really was able to spread significantly better than the other, then we would expect to see a difference here, and we don’t.”
Times of Israel also reported that “In late May researchers in University College London said their studies of the genomes of more than 15,000 samples had not shown one strain being more infectious than others.”
So, the jury’s out. Nonetheless, clinical laboratory leaders will want to remain vigilant. A sudden increase in COVID-19 infection rates will put severe strain on already strained laboratory supply chains.
It can take up to eight days after onset of symptoms for a person’s immune system to develop antibodies, so serological tests are not designed for diagnosing recent or active infections, stated a Mayo Clinic news story. However, Reuters reported that the availability of serological tests is “a potential game changer” because they could identify people who are immune even if they had no symptoms or only mild symptoms.
“Ultimately, this might help us figure out who can get the country back to normal,” Florian Krammer, PhD, told Reuters. Krammer’s lab at the Icahn School of Medicine at Mount Sinai in New York City has developed a serological test. “People who are immune could be the first people to go back to normal life and start everything up again,” he said.
However, some experts advise that the presence of antibodies is not necessarily a “get out of jail free” card when it comes to the coronavirus. “Infectious disease experts say immunity against COVID-19 may last for several months and perhaps a year or more based on their studies of other coronaviruses, including Severe Acute Respiratory Syndrome (SARS), which emerged in 2003,” reported Reuters. “But [the experts] caution that there is no way to know precisely how long immunity would last with COVID-19, and it may vary person to person.”
Additionally, it is also “uncertain whether antibodies would be sufficient protection if a person were to be re-exposed to the virus in very large amounts,” such as in an emergency room or ICU, Reuters reported.
Serological Survey Studies Get Underway Worldwide
Aside from detecting potential immunity, the World Health Organization (WHO) says serological tests could be useful for widespread disease surveillance and epidemiological research.
In the US, the Vitalant
Research Institute is leading several large serological survey or
“serosurvey” studies in which regional blood centers save samples of donated
blood for antibody testing, Science
reported.
Science also reported on a similar WHO initiative in which six countries will pool data from their own antibody studies. And in the Netherlands, blood banks have begun screening thousands of blood donations for presence of antibodies, Wired reported.
FDA Emergency Use Authorization
On March 16, the federal Food and Drug Administration (FDA) announced that it would allow commercial development and distribution of serological tests that “identify antibodies (e.g., IgM, IgG) to SARS-CoV-2 from clinical specimens” without an Emergency Use Authorization (EUA). The agency noted that these tests are “less complex than molecular tests” used to detect active infections, and that the policy change is limited to such testing in medical laboratories or by healthcare workers at the point-of-care. “This policy does not apply to at home testing,” the FDA reiterated.
“Serological tests can play a critical role in the fight against COVID-19 by helping healthcare professionals to identify individuals who have overcome an infection in the past and have developed an immune response,” said FDA Commissioner Stephen M. Hahn, MD (above with President Trump during a Coronavirus Task Force press briefing), in an April 7 press statement. “In the future, this may potentially be used to help determine—together with other clinical data—that such individuals are no longer susceptible to infection and can return to work. In addition, these test results can aid in determining who may donate a part of their blood called convalescent plasma, which may serve as a possible treatment for those who are seriously ill from COVID-19.” (Photo copyright: CNBC.)
FDA Issues First EUA for Rapid Diagnostic Test
Cellex Inc., based in Research Triangle Park, N.C., received the first EUA for its qSARS-CoV-2 serological test on April 1. As with other rapid diagnostic tests (RDTs) under development, the qSARS-CoV-2 test detects the presence of immunoglobulin M (IgM) and immunoglobulin G (IgG) antibodies in human blood. The biotechnology company’s RDT can be used to test serum, plasma, or whole-blood specimens, stated Cellex, and can produce results in 15 to 20 minutes.
The FDA has authorized use of the antibody test only by laboratories certified under CLIA to perform moderate and high complexity tests. Cellex has set up a COVID-19 website with information about the qSARS-CoV-2 test for clinical laboratories, patients, and healthcare providers.
Other Serological Tests Under Development
Mayo
Clinic Laboratories announced on April 13 that it is ramping up
availability of an internally-developed serological test. “Initial capacity
will be 8,000 tests per day performed at laboratory locations across Mayo Clinic,” stated the announcement.
“Testing will be performed 24 hours a day, and Mayo Clinic Laboratories is working
to ensure turnaround time is as close as possible to 24 hours after receipt of
the sample.”
Emory University in Atlanta announced on April 13 that it will begin deploying its own internally developed antibody test. Initially, testing will be limited to 300 people per day, comprised of Emory Healthcare patients, providers, and staff members. Eventually, testing will be “expanded significantly,” said Emory, with a goal of 5,000 tests per day by mid-June.
RDTs are typically qualitative, meaning they produce a
positive or negative result, stated the Center for Health Security. An ELISA
test “can be qualitative or quantitative,” noted the Center, but it can take
one to five hours to produce results.
A third type of serological test—the neutralization assay—involves infecting a patient’s blood with live coronavirus to determine if antibodies exist that can inhibit growth of the virus. The test takes three to five days in a level 3 biosafety laboratory to produce results. The Straits Times reported on one laboratory in Singapore that developed a neutralization assay to trace the source of COVID-19 infections that originated in Wuhan, China.
Serological testing is another important tool clinical
laboratories and epidemiologists can use to fight and ultimately defeat the
COVID-19 pandemic and is worth watching.
Asian locales reacted swiftly to the threat of COVID-19 by leveraging lessons learned from previous pandemics and making use of serology testing in aggressive contact tracing
America’s healthcare leaders in government, hospitals, clinical pathology, and medical laboratories can learn important lessons from the swift responses to the early outbreaks of COVID-19 in countries like Taiwan and South Korea and in cities like Singapore and Hong Kong.
Strategies such as early intervention, commitment to tracing contacts of infected people within two hours, quarantines, and social distancing all contributed to significantly curtailing the spread of the latest coronavirus pandemic within their borders, The New York Times (NYT) reported.
Another response common to the efforts of these countries and cities was the speedy introduction of clinical laboratory tests for SARS-CoV-2, the novel coronavirus that causes coronavirus disease 2019 (COVID-19), supported by the testing of tens of thousands of people in the earliest stages of the outbreaks in their communities. And that preparation and experience is paying off as those countries and cities continue to address the spread of COVID-19.
‘We Look at SARS as the Dress Rehearsal’
“Maybe it’s because of our Asian context, but our community
is sort of primed for this. We will keep fighting, because isolation and
quarantine work,” Lalitha
Kurupatham, Deputy Director of the Communicable Diseases Division in
Singapore, told the NYT. “During peacetime, we plan for epidemics like
this.”
Clinical laboratory leaders and pathologists may recall that Hong Kong was the site of the 2003 severe acute respiratory syndrome (SARS) epidemic. About 8,096 people worldwide were infected, and 774 died from SARS, according to the World Health Organization (WHO). In Hong Kong, 299 died out of 1,755 cases. However, Singapore had just 238 cases and 33 deaths.
To what does Singapore attribute the country’s lower
COVID-19 infection/death rate today?
“We can look at SARS as the dress rehearsal. The experience was raw, and very, very visceral. And on the back of it, better systems were put in place,” Jeremy Lim, MD, Co-Director of the Leadership Institute for Global Health Transformation at the National University of Singapore, told TIME.
“It’s a mix of carrots and sticks that have so far helped us. The US should learn from Singapore’s response and then adapt what is useful,” Lim added.
Singapore Debuts Serology Testing for COVID-19 Tracking
As microbiologists and infectious diseases doctors know, serology tests work by identifying antibodies that are the sources of infection. In the case of COVID-19, these tests may have aided in the surveillance of people infected with the coronavirus.
This is one lesson the US is learning.
“CDC (Centers for Disease Control and Prevention) has developed two serological tests that we’re evaluating right now, so we can get an idea through surveillance what’s the extent of this outbreak and how many people really are infected,” Robert Redfield, MD, CDC Director, told STAT.
The graphic above, which is based on data from the federal Centers for Disease Control and Prevention, illustrates how contact tracing is accomplished. “We believe this is the first time in the world where these particular tests have been used in this context of contact tracing,” Danielle Anderson, PhD, Scientific Director, Duke-NUS Medical School ABSL3 Laboratory, told Science. (Graphic copyright: CDC/Carl Fredrik Sjöland.)
‘Leaving No Stone Unturned’
As of March 27, Singapore (located about 2,374 miles from
mainland China with a population of 5.7 million) had reported 732 COVID-19
cases and two deaths, while Hong Kong had reported 518 cases and four deaths.
According to Time, in its effort to battle and treat
COVID-19, Singapore took the following steps:
Clinical laboratory testing for COVID-19 of all
people presenting with “influenza-like” and pneumonia symptoms;
Contact tracing of each infected person,
including interviews, review of flight manifests, and police involvement;
Using locally developed test to find antibodies
after COVID-19 clears;
Ran ads on page one of newspapers urging people
with mild symptoms to see a doctor; and
Government paid $100 Singapore dollars per day to
quarantined self-employed people.
The Singapore government’s WhatsApp account shares updates on the coronavirus, and Singapore citizens acquire wearable stickers after having their temperature checked at building entrances, Wired reported. The article also noted teams of healthcare workers are kept separate in hospitals—just in case some workers have to be quarantined.
FREE Webinar | What Hospital and Health System Labs Need to Know About Operational Support and Logistics During the COVID-19 Outbreak Wednesday, April 1, 2020 @ 1PM EDT — Register Now
Meanwhile, in Hong Kong, citizens donned face masks and
pressured the government to respond to the COVID-19 outbreak. Officials subsequently
tightened borders with mainland China and took other action, the NYT reported.
Once the COVID-19 genetic sequence became available, national medical laboratory networks in Singapore, Hong Kong, and Japan developed their own diagnostic tests, reported The Lancet, which noted that the countries also expanded capacity for testing and changed financing systems, so people would not have to pay for the tests. In Singapore, the government pays for hospitalization as well, noted The Lancet.
Lessons Learned
The US has far less experience with pandemics, as compared to the Asian locales that were affected by the H1N1 influenza (Spanish Flu) of 1918-1920 and the H5N1 influenza (Avian Flu) of 1957-1958.
And, controversially, National Security Council (NSC) officials in 2018 discontinued the federal US Pandemic Response Unit, moving the NSC employees into other government departments, Associated Press reported.
According to the March 26 US Coronavirus Task Force’s televised
news conference, 550,000 COVID-19 tests have been completed nationwide and
results suggest 86% of those tested are negative for the disease.
The fast-moving virus and rapidly developing story are placing
medical laboratory testing in the global spotlight. Pathologists and clinical laboratory
leaders have a unique opportunity to advance the profession, as well as improving
the diagnosis of COVID-19 and the health of patients.
By taking early measures to combat the spread, the country had a medical laboratory test for COVID-19 available as early as Jan. 24, and was able to focus medical laboratory testing on the most at-risk individuals
With the Coronavirus disease 2019 (COVID-19) outbreak dominating headlines and medical laboratories under growing pressure to increase testing capacity, Taiwan’s rapid response to the pandemic could provide a critical model for other countries to follow.
Given its proximity to mainland China—just 81 miles—and the large number of individuals who frequently travel back and forth between the countries, Taiwan was at risk of having the second-highest number of imported COVID-19 cases, according to a model developed by researchers at Johns Hopkins University and the University of New South Wales Sydney. News reports indicate that, each year, about 60,000 flights carry 10 million passengers between Taiwan and China.
Data from Taiwan’s Centers for Disease Control (CDC) and Central Epidemic Command Center (CECC) indicate that the country has managed to contain the outbreak thanks to these aggressive actions.
As of March 19, Taiwan’s CECC reported a total of 108 laboratory-confirmed COVID-19 infections. That compares with 81,155 in China, 41,035 in Italy, and 10,755 in the US, according to data compiled by the Center for Systems Science and Engineering at Johns Hopkins University. When the World Health Organization (WHO) reports on the number of COVID-19 cases by country, it includes the number of COVID-19 cases from Taiwan under the totals for the People’s Republic of China. WHO made this decision several years ago, under pressure by China to not recognize Taiwan as an independent nation.
The World
Population Review website says Taiwan’s population is about 23.8 million.
But its infection rate is low even on a per capita basis: Approximately 45
infections per million population, compared with 6,784 in Italy, 564 in China,
and 326 per million in the US.
The JAMA authors noted that Taiwan was prepared for
an outbreak after its experience with the severe
acute respiratory syndrome (SARS) pandemic in 2003, which also originated
in China.
Timeline of COVID-19 Outbreak at the Earliest Stages
Taiwan apparently learned a lesson about preparedness from
the SARS outbreak the rest of the world did not and that enabled the tiny
nation to respond immediately to the novel Coronavirus threat.
The country’s efforts began on Dec. 31 with inspections of
flight arrivals from Wuhan. “When there were only a very few cases [of
COVID-19] reported in China, [Taiwanese health authorities] already went onto
every airplane that came from Wuhan,” C. Jason Wang,
MD, PhD, an Associate Professor of Pediatrics and Director of the Center for Policy, Outcomes, and
Prevention at Stanford University and lead author of the JAMA
report, told Vox.
“Health officials came on the airplane and checked people for symptoms,” he
added.
Travelers who had recently visited Wuhan and displayed
symptoms of pneumonia were quarantined at home for 14 days. Taiwan’s
CDC reported that quarantined individuals were being tested for the
2019-nCoV coronavirus (later renamed to SARS-CoV-2)
soon after it was identified. The CECC, activated in January to coordinate the
government’s response, reported the first confirmed imported case on Jan. 21.
On Jan. 24, their
CDC announced that testing for the virus was being performed at the CDC and
eight designated hospitals. Testing included samples from physicians around the
country. As of Feb. 17, daily testing capacity was about 1,300 samples, the JAMA
authors reported.
Wang told Vox that aggressive measures to identify
and isolate at-risk individuals at the earliest stages reduced the volume of clinical
laboratory tests that had to be performed. “Here in the US and elsewhere, we’re
now seeing community spread,” he said. “It’s probably been here for a while.
And so now we’re trying to see, ‘Oh, how many people should we test?’ Then, you
really need to have a very large capacity in the beginning.”
“I think the US has enormous capacity that’s currently not being used,” C. Jason Wang, MD, PhD (above), Associate Professor of Pediatrics and Director of the Center for Policy, Outcomes, and Prevention at Stanford University and lead author of the JAMA report, told Vox. “We have big tech companies that really could do a lot, right? We ought to get the big companies together. Get the governors together, get the federal government agencies to work with each other, and try to find innovative ways to think about how to best do this. We’ve got the smartest people here in the US because they come from everywhere. But right now, those are untapped resources. They’re not working together. And the federal government, the agencies, they need to collaborate a little more closely.” (Photo copyright: Stanford University.)
More Actions by Authorities
The JAMA report supplementary materials notes a total of 124 actions taken by Taiwanese authorities between Jan. 20 and Feb. 24 to contain the outbreak. In addition to the border inspections, quarantines and testing, they included integration of data between the country’s National Health Insurance Administration and National Immigration Agency, so authorities, and later hospitals, could identify any patient who had recently traveled to China, Hong Kong, or Macau.
The steps also included:
An escalating series of travel restrictions,
eventually including suspension of most passenger flights from Taiwan to China,
as well as a suspension of tours to Hong Kong or Macau.
Use of government-issued cell phones to monitor
quarantined individuals.
Fines for individuals breaking the 14-day home
quarantine.
Fines for incoming travelers who failed to
provide accurate health information.
Fines for disseminating false information or
rumors about the epidemic.
Fines and jail sentences for profiteering on disease-prevention
products.
Designation of military camps and other
government facilities for quarantine.
Nationwide disinfection of universities,
colleges, and public spaces around schools.
The government also took aggressive action to ensure
adequate supplies of surgical masks, including stepped-up manufacturing, export
bans, price limits, and a limit of one to three masks per purchase.
The JAMA authors noted that government officials issued daily press briefings to educate the public about the outbreak. Communication efforts also included public service announcements by Taiwan Vice President Chen Chien-jen, a trained epidemiologist.
A poll taken in Taiwan on Feb. 17 and 18 indicated high approval ratings for officials’ response to the crisis.
The JAMA authors also noted some “challenges” in the
government’s response. For example, most real-time public communication was in
Mandarin Chinese and sign language, leaving out non-Taiwanese citizens in the
country. And the cruise ship Diamond Princess, later found to have infections
on board, was allowed to dock near Taipei and disembark passengers. There are
also questions about whether similar policies can be sustained through the end
of a pandemic.
Still, “well-trained and experienced teams of officials were
quick to recognize the crisis and activated emergency management structures to
address the emerging outbreak,” the JAMA authors wrote. “Taiwan is an
example of how a society can respond quickly to a crisis and protect the
interests of its citizens.”
One noteworthy difference in the speedy response to
recognition of a novel coronavirus in Taiwan, compared to recognition of the
same novel coronavirus in the United States, was the fast availability of
clinical laboratory tests for COVID-19 in Taiwan.
Pathologists and clinical laboratory professionals here in
the US are frustrated that their skills and talents at developing and
validating new assays on an accelerated timeline were not acknowledged and
leveraged by government officials as they decided how to respond to the
emergence of the novel coronavirus now called SARS-CoV-2.
As standard masks are used they collect exhaled airborne pathogens that remain living in the masks’ fibers, rendering them infectious when handled
Surgical-style facial masks harbor a secret—viruses that could be infectious to the people wearing them. However, masks can become effective virus killers as well. At least that’s what researchers at the University of Alberta (UAlberta) in Edmonton, Canada, have concluded.
If true, such a re-engineered mask could protect clinical laboratory workers from exposure to infectious diseases, such as, SARS (Severe Acute Respiratory Syndrome), MERS (Middle East Respiratory Syndrome), and Swine Influenza.
“Surgical masks were originally designed to protect the wearer from infectious droplets in clinical settings, but it doesn’t help much to prevent the spread of respiratory diseases such as SARS or MERS or influenza,” Hyo-Jick Choi, PhD, Assistant Professor in UAlberta’s Department of Chemical and Materials Engineering, noted in a press release.
So, Choi developed a mask that effectively traps and kills airborne viruses.
Clinical Laboratory Technicians at Risk from Deadly Infectious Diseases
The global outbreak of SARS in 2003 is a jarring reminder of how infectious diseases impact clinical laboratories, healthcare workers, and patients. To prevent spreading the disease, Canadian-based physicians visited with patients in hotel rooms to keep the virus from reaching their medical offices, medical laboratory couriers were turned away from many doctors’ offices, and hospitals in Toronto ceased elective surgery and non-urgent services, reported The Dark Report—Dark Daily’s sister publication. (See The Dark Report, “SARS Challenges Met with New Technology,” April 14, 2003.)
UAlberta materials engineering professor Hyo-Jick Choi, PhD, (right) and graduate student Ilaria Rubino (left) examine filters treated with a salt solution that kills viruses. Choi and his research team have devised a way to improve the filters in surgical masks, so they can trap and kill airborne pathogens. Clinical laboratory workers will especially benefit from this protection. (Photo and caption copyright: University of Alberta.)
How Current Masks Spread Disease
How do current masks spread infectious disease? According to UAlberta researchers:
A cough or a sneeze transmits airborne pathogens such as influenza in aerosolized droplets;
Virus-laden droplets can be trapped by the mask;
The virus remains infectious and trapped in the mask; and,
Risk of spreading the infection persists as the mask is worn and handled.
“Aerosolized pathogens are a leading cause of respiratory infection and transmission. Currently used protective measures pose potential risk of primary and secondary infection and transmission,” the researchers noted in their paper, published in Scientific Reports.
That’s because today’s loose-fitting masks were designed primarily to protect healthcare workers against large respiratory particles and droplets. They were not designed to protect against infectious aerosolized particles, according to the Centers for Disease Control and Prevention (CDC).
In fact, the CDC informed the public that masks they wore during 2009’s H1N1 influenza virus outbreak provided no assurance of infection protection.
“Face masks help stop droplets from being spread by the person wearing them. They also keep splashes or sprays from reaching the mouth and nose of the person wearing the face mask. They are not designed to protect against breathing in very small particle aerosols that may contain viruses,” a CDC statement noted.
Pass the Salt: A New Mask to Kill Viruses
Choi and his team took on the challenge of transforming the filters found on many common protective masks. They applied a coating of salt that, upon exposure to virus aerosols, recrystallizes and destroys pathogens, Engineering360 reported.
“Here we report the development of a universal, reusable virus deactivation system by functionalization of the main fibrous filtration unit of surgical mask with sodium chloride salt,” the researchers penned in Scientific Reports.
The researchers exposed their altered mask to the influenza virus. It proved effective at higher filtration compared to conventional masks, explained Contagion Live. In addition, viruses that came into contact with the salt-coated fibers had more rapid infectivity loss than untreated masks.
How Does it Work?
Here’s how the masks work, according to the researchers:
Aerosol droplets carrying the influenza virus contact the treated filter;
The droplet absorbs salt on the filter;
The virus is exposed to increasing concentration of salt; and,
The virus is damaged when salt crystallizes.
“Salt-coated filters proved highly effective in deactivating influenza viruses regardless of [influenza] subtypes,” the researchers wrote in Scientific Reports. “We believe that [a] salt-recrystallization-based virus deactivation system can contribute to global health by providing a more reliable means of preventing transmission and infection of pandemic or epidemic diseases and bioterrorism.”
Other Reports on Dangerous Exposure for Clinical Laboratory Workers
This is not the first time Dark Daily has reported on dangers to clinical laboratory technicians and ways to keep them safe.
In “Health of Pathology Laboratory Technicians at Risk from Common Solvents like Xylene and Toluene,” we reported on a 2011 study that determined medical laboratory technicians who handle common solvents were at greater risk of developing auto-immune connective tissue diseases.
The UAlberta team may have come up with an inexpensive, simple, and effective way to protect healthcare workers and clinical laboratory technicians. Phlebotomists, laboratory couriers, and medical technologists also could wear the masks as protection from accidental infection and contact with specimens. It will be interesting to follow the progress of this special mask with its salty filter.