Findings may lead to new clinical laboratory biomarkers for predicting risk of developing MS and other autoimmune diseases
Scientists continue to find new clinical laboratory biomarkers to detect—and even predict risk of developing—specific chronic diseases. Now, in a recent study conducted at the University of California San Francisco (UCSF), researchers identified antibodies that develop in about 10% of Multiple Sclerosis (MS) patients’ years before the onset of symptoms. The researchers reported that of those who have these antibodies, 100% develop MS. Thus, this discovery could lead to new blood tests for screening MS patients and new ways to treat it and other autoimmune diseases as well.
The UCSF researchers determined that, “in about 10% [of] cases of multiple sclerosis, the body begins producing a distinctive set of antibodies against its own proteins years before symptoms emerge,” Yahoo Life reported, adding that “when [the patients] are tested at the time of their first disease flare, the antibodies show up in both their blood and cerebrospinal fluid.”
That MS is so challenging to diagnose in the first place makes this discovery even more profound. And knowing that 100% of a subset of MS patients who have these antibodies will develop MS makes the UCSF study findings quite important.
“This could be a useful tool to help triage and diagnose patients with otherwise nonspecific neurological symptoms and prioritize them for closer surveillance and possible treatment,” Colin Zamecnik, PhD, scientist and research fellow at UCSF, told Yahoo Life.
“From the largest cohort of blood samples on Earth, we obtained blood samples from MS patients years before their symptoms began and profiled antibodies against self-autoantibodies that are associated with multiple sclerosis diagnosis,” Colin Zamecnik, PhD (above), scientist and research fellow at UCSF, told Yahoo Life. “We found the first molecular marker of MS that appears up to five years before diagnosis in their blood.” These findings could lead to new clinical laboratory tests that determine risk for developing MS and other autoimmune diseases. (Photo copyright: LinkedIn.)
UCSF Study Details
According to the MS International Foundation Atlas of MS, there are currently about 2.9 million people living with MS worldwide, with about one million of them in the US. The disease is typically diagnosed in individuals 20 to 50 years old, mostly targeting those of Northern European descent, Yahoo Life reported.
To complete their study, the UCSF scientists used the Department of Defense Serum Repository (DoDSR), which is comprised of more than 10 million individuals, the researchers noted in their Nature Medicine paper.
From that group, the scientists identified 250 individuals who developed MS, spanning a period of five years prior to showing symptoms through one year after their symptoms first appeared, Medical News Today reported. These people were compared to 250 other individuals in the DoDSR who have no MS diagnosis but who all had similar serum collection dates, ages, race and ethnicities, and sex.
“The researchers validated the serum results against serum and cerebrospinal fluid results from an incident MS cohort at the University of California, San Francisco (ORIGINS) that enrolled patients at clinical onset. They used data from 103 patients from the UCSF ORIGINS study,” according to Medical News Today. “They carried out molecular profiling of autoantibodies and neuronal damage in samples from the 500 participants, measuring serum neurofilament light chain measurement (sNfL) to detect damage to nerve cells.
“The researchers tested the antibody patterns of both MS and control participants using whole-human proteomeseroreactivity which can detect autoimmune reactions in the serum and CSF,” Medical News Today noted.
Many who developed MS had an immunogenicity cluster (IC) of antibodies that “remained stable over time” and was not found in the control samples. The higher levels of sNfL in those with MS were discovered years prior to the first flare up, “indicating that damage to nerve cells begins a long time before symptom onset,” Medical News Today added.
“This signature is a starting point for further immunological characterization of this MS patient subset and may be clinically useful as an antigen-specific biomarker for high-risk patients with clinically or radiologically isolated neuroinflammatory syndromes,” the UCSF scientists wrote in Nature Medicine.
“We believe it’s possible that these patients are exhibiting cross reactive response to a prior infection, which agrees with much current work in the literature around multiple sclerosis disease progression,” Zamecnik told Yahoo Life.
It “validates and adds to prior evidence of neuro-axonal injury occurring in patients during the MS preclinical phase,” the researchers told Medical News Today.
Implications of UCSF’s Study
UCSF’s discovery is a prime example of technology that could soon work its way into clinical use once additional studies and research are done to support the findings.
The researchers believe their research could lead to a simple blood test for detecting MS years in advance and discussed how this could “give birth to new treatments and disease management opportunities,” Neuroscience News reported.
Current MS diagnosis requires a battery of tests, such as lumbar punctures for testing cerebrospinal fluid, magnetic resonance imaging (MRI) scans of the spinal cord and brain, and “tests to measure speed and accuracy of nervous system responses,” Medical News Today noted.
“Given its specificity for MS both before and after diagnosis, an autoantibody serology test against the MS1c peptides could be implemented in a surveillance setting for patients with high probability of developing MS, or crucially at a first clinically isolated neurologic episode,” the UCSF researchers told Medical News Today.
The UCSF discovery is another example of nascent technology that could work its way into clinical use after more research and studies. Microbiologists, clinical laboratories, and physicians tasked with diagnosing MS and other autoimmune diseases should find the novel biomarkers the researchers identified most interesting, as well as what changed with science and technology that enabled researchers to identify these biomarkers for development.
Multiple studies have shown that people with darker skin pigmentation run a higher risk of being misdiagnosed and undertreated than patients with lighter skin due to inaccurate oxygen level readings
Now, scientists at multiple institutions are working to improve the basic pulse oximeter’s design by making it capable of measuring multiple biomarkers, as well as addressing long-standing inaccuracies in the device when used on people with darker skin pigmentation.
This ongoing research demonstrates how new technologies are enabling innovators to add useful functions to standard, well-accepted devices.
Valencia Koomson, PhD (above), Associate Professor, Electrical and Computer Engineering, and head of the Advanced Integrated Circuits and Systems Lab at Tufts University, has developed a pulse oximeter that measures oxygenation in tissue, rather than in blood. Her approach could ensure patients with darker skin pigmentation will be accurately diagnosed at the point-of-care. Though generally not used in clinical laboratory settings, medical technologists will be interested to learn of these new innovations in pulse oximeters. (Photo copyright: Tufts University.)
Measuring Tissues Instead of Blood
The pulse oximeter—a device that attaches to a person’s finger—uses red and infrared light to measure blood oxygen saturation (SpO2) and display pulse rate.
Studies in 2022 that looked into how hospitals administered oxygen to different patients found that inconsistent pulse oximeter readings could cause caregivers to administer less oxygen than is actually needed to people with darker skin pigmentation.
This is because melanin in the skin can interfere with “absorption of light used to measure oxygenated blood in a person’s finger,” according to a National Science Foundation (NSF) news story. Such inaccurate pulse oximeter readings can lead to “inaccurate readings and poorer treatment outcomes” for people with dark skin tones, the NSF wrote.
“Addressing this problem will require innovation in pulse oximeter design and revised regulatory standards,” said Valencia Koomson, PhD, Associate Professor, Electrical and Computer Engineering, Tufts University, Medford, Massachusetts, in the NSF news story.
Koomson, who leads the Advance Integrated Circuit and Systems Lab at Tufts, has developed a prototype pulse oximeter device, which NSF explained, measures oxygenation in biological tissues instead of blood.
“My lab’s work on pulse oximeter devices will provide an alternative technology to address many confounding factors that affect pulse oximeter accuracy, including skin pigmentation, motion artifact, and others,” Koomson said.
National Public Radio (NPR) said Koomson’s device has built-in “technology that can measure a person’s skin tone.”
“We can send more light if there’s a higher level of melanin present, so that melanin doesn’t become a confounding factor that obscures our results,” Koomson told NPR.
Another Pulse Oximeter Redesign
Another new approach to pulse oximetry was developed at Brown University in Providence, Rhode Island.
Rutendo Jakachira, Research Assistant, School of Engineering, and a PhD student in physics, turned to new optical techniques to address the challenge of oxygen saturation levels in dark skin tones, according to a Brown University news release.
Jakachira and Kimani Toussaint, PhD, Professor of Engineering and Senior Associate Dean in the School of Engineering, say they have created possibly the first LED-based light source to emit radially polarized light.
When the LED passes light through a person’s finger, the device calculates the amount of light the hemoglobin in the blood absorbed, NPR explained.
“We did a preliminary study on about five people, and although it was a small study, the results are promising,” said Jakachira, who plans a larger study and clinical trial.
Study Suggests Patients with Darker Skin May Have Received Delayed COVID-19 Care
The researchers analyzed electronic health record (EHR) data from 43,753 patients at Sutter Health in Sacramento, California, who had SpO2 measurements done between January 2020 and February 2022, and 8,735 patients seen for COVID-19 between July 2020 and February 2021 in the hospital’s emergency department.
In their AJE paper, they wrote, “We investigated whether or not pulse oximetry systematically underestimated oxygen saturation in patients who identified as NHB [non-Hispanic Black/African-American] as compared with NHW [non-Hispanic White] counterparts. We also assessed whether or not differences in oxygen saturation measurement affected hospital admission, care delivered, or return to the hospital post discharge among patients with COVID-19.
“We found evidence of differential pulse oximeter measurement error in NHB individuals, resulting in nonrandom overestimation of blood oxygenation as compared with NHW individuals. NHB individuals were also more likely to have hypoxemia [abnormally low oxygen levels in the blood] not detected by pulse oximetry.
“For NHB patients presenting in the ED with COVID-19, we found that overestimation of oxygen saturation was associated with underestimation of the need for admission and underestimation of the need for treatment with dexamethasone and supplemental oxygen. Additionally, we observed associated delays in dexamethasone initiation and initiation of oxygen supplementation.
“There are also broader implications beyond COVID-19, as differential pulse oximeter accuracy has the potential to exacerbate disparities for any condition that relies upon blood oxygenation measurement to inform clinical decision-making.”
Importance of Accurate Readings
Developing pulse oximeters that are accurate for all people, regardless of skin tone, is clearly an important breakthrough. Medical laboratory leaders and pathologists recognize that SpO2 data—along with clinical laboratory test results—are critical for successful diagnostics and treatment. Thus, new technologies that add useful functions to well-accepted devices are positive developments and worth watching.
Understanding why some people display no symptoms during a COVID-19 infection could lead to new precision medicine genetic tests medical labs could use to identify people with the mutated gene
New research from the University of California San Francisco (UCSF) may explain why some people could get COVID-19 but never test positive on a clinical laboratory test or develop symptoms despite exposure to the SARS-CoV-2 coronavirus.
According to the UCSF study, variations in a specific gene in a system of genes responsible for regulating the human immune system appears to be the factor in why about 10% of those who become infected with the virus are asymptomatic.
These scientific insights did not receive widespread news coverage but will be of interest to clinical laboratory managers and pathologists who oversee SARS-CoV-2 testing in their labs.
“Some people just don’t have symptoms at all,” Jill Hollenbach, PhD (above), Professor of Neurology atUCSF’s Weill Institute for Neurosciences and lead researcher in the study, told NBC News. “There’s something happening at a really fundamental level in the immune response that is helping those people to just completely wipe out this infection.” Identifying a genetic reason why some people are asymptomatic could lead to new precision medicine clinical laboratory diagnostics for COVID-19. (Photo copyright: Elena Zhukova /University of California San Francisco.)
Fortunate Gene Mutation
According to the Centers for Disease Control and Prevention’s (CDC) COVID Data Tracker, as of April 5, 2023, a total of 104,242,889 COVID-19 cases have been reported in the United States. However, according to a CDC Morbidity and Mortality Weekly Report (MMWR), “Traditional methods of disease surveillance do not capture all COVID-19 cases because some are asymptomatic, not diagnosed, or not reported; therefore, [knowing the true] proportion of the population with SARS-CoV-2 antibodies (i.e., seroprevalence) can improve understanding of population-level incidence of COVID-19.”
She also participates in the COVID-19 HLA and Immunogenetics Consortium, a group of academic researchers, clinical laboratory directors, journal editors, and others who examine the role of HLA variations in determining COVID-19 risk.
Hollenbach’s research identified an HLA variant—known as HLA-B*15:01—that causes the human immune system to react quickly to SARS-CoV-2 and “basically nuke the infection before you even start to have symptoms,” she told NPR.
“It’s definitely luck,” she added. “But, you know, this [gene] mutation is quite common. We estimate that maybe one in 10 people have it. And in people who are asymptomatic, that rises to one in five.”
“HLA variants are among the strongest reported associations with viral infections,” the UCSF study notes. So, the researchers theorized that HLA variations play a role in asymptomatic SARS-CoV-2 infections as well.
To conduct their study, shortly after the SARS-CoV-2 outbreak in 2020, the researchers recruited approximately 30,000 volunteer bone marrow donors from the National Marrow Donor Program to respond to periodic questions via a smartphone app or website. Because HLA variations can determine appropriate matches between donors and recipients, the database includes information about their HLA types.
Each week, respondents were asked to report if they had been tested for SARS-CoV-2. Each day, they were asked to report whether they had symptoms associated with COVID-19. “We were pretty stringent in our definition of asymptomatic,” Hollenbach told NBC News. “[The respondents couldn’t] even have a scratchy throat.”
The researchers eventually identified a cohort of 1,428 people who had tested positive for SARS-CoV-2 between February 2020 and April 30, 2021, before vaccines were widely available. Among these individuals, 136 reported no symptoms for two weeks before or two weeks after a positive test.
“Overall, one in five individuals (20%) who remained asymptomatic after infection carried HLA-B*15:01, compared to 9% among patients reporting symptoms,” the researchers wrote in their medRxiv preprint. Study participants with two copies of the gene were more than eight times more likely to be asymptomatic.
The UCSF researchers also looked at four other HLA variants and found none to be “significantly associated” with lack of symptoms. They confirmed their findings by reproducing the HLA-B association in two additional independent cohorts, one from an earlier study in the UK and the other consisting of San Francisco-area residents.
Individuals in the latter group had either tested positive for SARS-CoV-2 or reported COVID symptoms, and their DNA was analyzed to determine their HLA types.
Pre-existing T-Cell Immunity May Reduce Severity of COVID-19 Infection
The UCSF researchers also attempted to determine how HLA-B*15:01 plays a role in knocking out SARS-CoV-2 infections. They noted previous research that indicated previous exposure to seasonal coronaviruses, such as common cold viruses, could limit the severity of COVID-19. The scientists hypothesized that pre-existing T-cell immunity in HLA-B carriers may be the key.
The COVID-19 HLA and Immunogenetics Consortium website describes how HLA and T-cells work together to ward off disease. HLA “proteins are found on the surface of all cells except red-blood cells.” They’re “like windows into the inner workings of a cell,” and T-cells use the molecules to determine the presence of foreign proteins that are likely signs of infection. “Activated T-cells can kill infected cells, or activate B-cells, which produce antibodies in response to an infection,” the website explains.
Hollenbach’s research team analyzed T-cells from pre-pandemic individuals and observed that in more than half of HLA-B carriers, the T-cells were reactive to a SARS-CoV-2 peptide. The scientists corroborated the hypothesis by examining crystal structures of the HLA-B*15:01 molecule in the presence of coronavirus spike peptides from SARS-CoV-2 and two other human coronaviruses: OC43-CoV and HKU1-CoV.
“Altogether, our results strongly support the hypothesis that HLA-B*15:01 mediates asymptomatic COVID-19 disease via pre-existing T-cell immunity due to previous exposure to HKU1-CoV and OC43-CoV,” the researchers wrote.
Can Genes Prevent COVID-19 Infections?
Meanwhile, researchers at The Rockefeller University in New York City are attempting to go further and see if there are mutations that prevent people from getting infected in the first place. NPR reported that they were seeking participants for a study seeking to identify so-called “superdodger” genes.
Study participants identified as possibly having superdodger genes receive a kit designed to collect saliva samples, after which the researchers sequence the respondents’ genomes. “We hope that in a group of 2,000 to 4,000 people, some people will have genetic mutations that tell us why they’re resistant to infection,” Casanova told NPR.
All this genetic research is in very early stages. But results are promising and may lead to new precision medicine clinical laboratory tests for identifying people who are predisposed to having an asymptomatic response to COVID-19 infection. That in turn could help scientists learn how to moderate or even eliminate symptoms in those unfortunate people who suffer the typical symptoms of the disease.
Might clinical laboratories soon be called on to conduct mass testing to find people who show little or no symptoms even though they are infected with the coronavirus?
Clinical laboratory managers understand that as demand for COVID-19 testing exceeds supplies, what testing is done is generally performed on symptomatic patients. And yet, it is the asymptomatic individuals—those who are shown to be infected with the SARS-CoV-2 coronavirus, but who experience no symptoms of the illness—who may hold the key to creating effective treatments and vaccinations.
So, as the COVID-19 pandemic persists, scientists are asking why some people who are infected remain asymptomatic, while others die. Why do some patients get severely ill and others do not? Researchers at the University of California San Francisco (UCSF) and Stanford University School of Medicine (Stanford Medicine) are attempting to answer these questions as they investigate viral transmission, masking, immunity, and more.
And pressure is increasing on researchers to find the answer. According to Monica Gandhi, MD, MPH, an infectious disease specialist and Professor of Medicine at UCSF, millions of people may be asymptomatic and unknowingly spreading the virus. Gandhi is also Associate Division Chief (Clinical Operations/Education) of the Division of HIV, Infectious Diseases, and Global Medicine at UCSF’s Zuckerberg San Francisco General Hospital and Trauma Center.
“If we did a mass testing campaign on 300 million Americans right now, I think the rate of asymptomatic infection would be somewhere between 50% and 80% of cases,” she told UCSF Magazine.
On a smaller scale, her statement was borne out. In a study conducted in San Francisco’s Mission District during the first six weeks of the city’s shelter-in-place order, UCSF researchers conducted SARS-CoV-2 reverse transcription-PCR and antibody (Abbott ARCHITECT IgG) testing on 3,000 people. Approximately 53% tested positive for COVID-19 but had no symptoms such as fever, cough, and muscle aches, according to data reported by Carina Marquez, MD, UCSF Assistant Professor of Medicine and co-author of the study, in The Mercury News.
Pandemic Control’s Biggest Challenge: Asymptomatic People
In an editorial in the New England Journal of Medicine (NEJM), Gandhi wrote that transmission of the virus by asymptomatic people is the “Achilles heel of COVID-19 pandemic control.”
In her article, Gandhi compared SARS-CoV-2, the coronavirus that causes COVID-19, to SARS-CoV-1, the coronavirus that caused the 2003 SARS epidemic. One difference lies in how the virus sheds. In the case of SARS-CoV-2, that takes place in the upper respiratory tract, but with SARS-CoV-1, it takes place in the lower tract. In the latter, symptoms are more likely to be detected, Gandhi explained. Thus, asymptomatic carriers of the coronavirus may go undetected.
“Viral loads with SARS-CoV-1, which are associated with symptom onset, peak a median of five days later than viral loads with SARS-CoV-2, which makes symptom-based detection of infection more effective in the case of SARS-CoV-1,” Gandhi wrote. “With influenza, persons with asymptomatic disease generally have lower quantitative viral loads in secretions from the upper respiratory tract than from the lower respiratory tract and a shorter duration of viral shedding than persons with symptoms, which decreases the risk of transmission from paucisymptomatic persons.”
Rick Wright (above), an insurance broker in Redwood City, Calif., was infected with the COVID-19 coronavirus while aboard a Diamond Princess Cruise. He underwent 40 days of isolation, and though he consistently tested positive for the coronavirus, he experienced no symptoms of the illness. “I never felt sick. Not a cough, wheezing, headache. Absolutely nothing,” he told Mercury News. (Photo copyright: The Mercury News.)
Stanford Studies Immune Responses in COVID-19 Patients
Meanwhile, scientists at the Stanford University School of Medicine were on their own quest to find out why COVID-19 causes severe disease in some people and mild symptoms in others.
“One of the great mysteries of COVID-19 infections has been that some people develop severe disease, while others seem to recover quickly. Now, we have some insight into why that happens,” Bali Pulendran, PhD, Stanford Professor of Pathology, Microbiology, and Immunology and Senior Author of the study in a Stanford Medicine news release.
The Stanford research suggested that three molecules—EN-RAGE, TNFSF14, and oncostatin-M—“correlated with disease and increased bacterial products in human plasma” of COVID-19 patients.
“Our multiplex analysis of plasma cytokines revealed enhanced levels of several proinflammatory cytokines and a strong association of the inflammatory mediators EN-RAGE, TNFSF14, and OSM with clinical severity of the disease,” the scientists wrote in Science.
Pulendran hypothesized that the molecules originated in patients’ lungs, which was the infection site.
“These findings reveal how the immune system goes awry during coronavirus infections, leading to severe disease and point to potential therapeutic targets,” Pulendran said in the news release, adding, “These three molecules and their receptors could represent attractive therapeutic targets in combating COVID-19.”
Clinical Laboratories May Do More Testing of Asymptomatic People
The research continues. In a televised news conference, President Trump said COVID-19 testing plays an important role in “preventing transmission of the virus.” Clearly this is true and learning why some people who are infected experience little or no symptoms may be key to defeating COVID-19.
Thus, as the nation reopens, clinical laboratories may want to find ways to offer COVID-19 testing beyond hospitalized symptomatic patients and people who show up at independent labs with doctors’ orders. As supplies permit, laboratory managers may want to partner with providers in their communities to identify people who are asymptomatic and appear to be well, but who may be transmitting the coronavirus.
Study scientists identified several currently available drugs that could inhibit growth of these “streaming filaments,” which infected cells use to go after non-infected cells
Like a scene from a bad horror movie, scientists have discovered that SARS-CoV-2, the coronavirus responsible for the COVID-19 pandemic, may be even more sinister and macabre than previously thought. The new research findings will interest those pathologists and clinical laboratory professionals who want to understand how the coronavirus spreads once it enters the body.
Headed by scientists from the University of San Francisco (UCSF), a team of international researchers discovered that “when the SARS-CoV-2 virus infects a human cell, it sets off a ghoulish transformation,” reported the Los Angeles Times (LA Times).
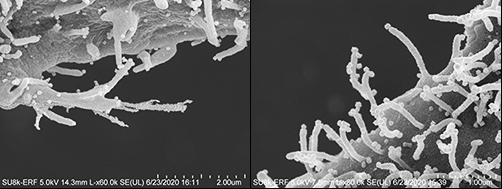
“Obeying instructions from the virus,” the LA Times continued, “the newly infected cell sprouts multi-pronged tentacles studded with viral particles. These disfigured zombie cells appear to be using those streaming filaments, or filopodia, to reach still-healthy neighboring cells. The protuberances appear to bore into the cells’ bodies and inject their viral venom directly into those cells’ genetic command centers—thus creating another zombie.”
As If the Coronavirus Weren’t Bad Enough!
“It’s just so sinister that the virus uses other mechanisms to infect other cells before it kills the cell,” Nevan Krogan, PhD, Professor, Department of Cellular Molecular Pharmacology at the UCSF School of Medicine, one of the study’s authors, told the LA Times.
The images above taken with an electron microscope show the streaming filaments—or as the researchers described in their published study, “filopodial protrusions possessing budding viral particles”—reaching out from cells infected with the SARS-CoV-2 coronavirus looking for other cells to infect. (Photos copyright: Los Angeles Times/Elizabeth Fischer, MA, Chief, RML Microscopy Unit, NIAID/NIH.)
SARS-CoV-2 Has Evolved, Study Suggests
Prior to this discovery, scientists believed that the coronavirus infected cells in a typical fashion by finding receptors on the surface of cells lining an individual’s mouth, nose, respiratory tract, lungs or blood vessels, and eventually replicating and invading larger cells. However, this new research may suggest that the virus has evolved and developed new ways to pass quickly and effectively from cell to cell.
While some other illnesses, including smallpox, human immunodeficiency virus (HIV), and some influenza viruses have been known to use filopodia to enhance their ability to infect cells, Krogan contends that those other viruses do not seem to have the prolific growth of the SARS-CoV-2 filopodia.
“By conducting a systematic analysis of the changes in phosphorylation when SARS-CoV-2 infects a cell, we identified several key factors that will inform not only the next areas of biological study, but also treatments that may be repurposed to treat patients with COVID-19,” he said, in a UCSF news release.
UCSF Study Identifies Drugs, Compounds That May Disrupt Growth of Filopodia
One key finding is that the coronavirus was utilizing a specific type of molecule from a family of cellular helpers known as Kinase to create the filopodia.
The researchers conducted a “quantitative mass spectrometry-based phosphoproteomics survey of SARS-CoV-2 infection in Vero E6 cells,” the study noted, which revealed a “dramatic rewiring of phosphorylation on host and viral proteins.
“SARS-CoV-2 infection promoted casein kinase 2 (CK2) and p38 MAPK activation, production of diverse cytokines, and shutdown of mitotic kinases, resulting in cell cycle arrest,” the study continued, adding, “Infection also stimulated a marked induction of CK2-containing filopodial protrusions possessing budding viral particles.
“Eighty-seven drugs and compounds were identified by mapping global phosphorylation profiles to dysregulated kinases and pathways. We found pharmacologic inhibition of the p38, CK2, CDK, AXL, and PIKFYVE kinases to possess antiviral efficacy, representing potential COVID-19 therapies,” the researchers concluded.
To determine if they might be helpful in combating COVID-19, the UCSF research team tested drugs and compounds that were either already cleared to market by the US federal Food and Drug Administration (FDA), in clinical trials, or under preclinical development.
After discovering the Kinase connection, the scientists focused on specialized drugs known as Kinase inhibitors.
“We narrowed in on about a dozen, and we highlighted about six or seven that look particularly potent in a laboratory setting,” Krogan told ABC News. “And we’re very excited now to try and take these into clinical trials.”
Among the drugs the study identified as potentially being able to disrupt the creation of filopodia and slow the spread of COVID-19 in the body are:
Silmitasertib: A drug that is currently in the clinical trial stages as a treatment for bile duct cancer and other cancers, including hematological and lymphoid malignancies;
“We are encouraged by our findings that drugs targeting differentially phosphorylated proteins inhibited SARS-CoV-2 infection in cell culture,” said Kevan Shokat, PhD, Professor of Cellular and Molecular Pharmacology at UCSF, and co-author of the study, in the UCSF news release. “We expect to build upon this work by testing many other kinase inhibitors, while concurrently conducting experiments with other technologies to identify underlying pathways and additional potential therapeutics that may intervene in COVID-19 effectively.”
Presently, the UCSF study provides no direct benefit to COVID-19 illness patients or clinical laboratories performing SARS-CoV-2 testing. However, that could change rapidly. Pathologists and medical laboratory managers will want to keep an eye on this research, because it may lead to new treatments for COVID-19 that would require increased clinical laboratory testing to identify people infected with the coronavirus.