Though coronavirus infections were detected nearly simultaneously in both Canada and the US, total cases and total deaths vary dramatically leading experts to question how differences in healthcare systems might have contributed
Can clinical laboratories in the United States learn from Canada’s response to the COVID-19 pandemic? While our northern neighbor won praise for its early response to the coronavirus, since then Canada has faced criticism over a lack of access to SARS-CoV-2 testing and long wait times for test results—criticism levied at the United States’ response to the outbreak as well.
In “Canada Shows How Easy Virus Testing Can Be,” Foreign Policy reported that Canada was more prepared to mount a successful response to COVID-19 because it systematically improved its pandemic-response preparedness and testing capacity after the 2003 SARS coronavirus (SARS-CoV-1) outbreak.
“Provincial laboratories put the infrastructure in place that would allow them to run their own testing and validation without help from the federal government,” Foreign Policy wrote. “At the same time, the federally run National Microbiology Laboratory in Winnipeg expanded its own capacity to support those efforts.”
However, Canada’s pandemic response has not been criticism free. In “Health Minister Says Test Result Wait Times ‘Not Acceptable’ As Ontario Confirms 25 New COVID-19 Cases,” CBC News reported in late March about COVID-19 testing shortages and four-day wait times for test results that were “not acceptable,” particularly in Ontario, where people with mild symptoms were being refused testing and sent home unless they worked in high-risk settings.
Government Bureaucracy’s Effect on Response to COVID-19
In “Canada’s Coronavirus Response Has Not Been Perfect. But It’s Done Far Better than the US,” The Washington Post reported that the initial exposure to the virus by the US and Canada was similar. Both the US and Canada have extensive ties to Europe and China, resulting in the two countries identifying their first cases of COVID-19 within a week of one another in January. Since then, however, the progression of the disease diverged dramatically in the two nations.
To date, the US has experienced 7,361,611 total cases with 209,808 total deaths, placing it in the number one spot globally on Worldometers’ COVID-19 tracking site. By contrast, Canada is in 26th place, with 155,301 total cases and 9,278 total deaths. However, to date the US has conducted 105,401,706 total clinical laboratory tests, as opposed to Canada’s 7,220,108 total tests. This might account for the disparity in total cases, but what accounts for the huge difference in total US deaths due to COVID-19 compared to Canada?
A Fraser Institute blog post authored by Steven Globerman, PhD, Resident Scholar and Addington Chair in Measurement at the Institute and Professor Emeritus at Western Washington University, titled, “US COVID Experience Highlights Risks of Centralized Management of Healthcare,” blamed the US’ “top-down, centralized approach to testing” for the “testing fiasco” that marked the US’ initial slow response to the pandemic. Globerman maintained the Centers for Disease Control and Prevention’s insistence on producing its own COVID-19 diagnostic test, rather than using a proven German-produced test, was the first of several missteps by the US.
“While there has been much criticism of the decentralized private insurance industry in the US, the major shortcomings in testing that characterize the US experience during the current pandemic seem to be the result of the government healthcare bureaucracy,” wrote Steven Globerman, PhD, (above), Resident Scholar and Addington Chair in Measurement at the Fraser Institute and Professor Emeritus at Western Washington University. (Photo copyright: Fraser Institute.)
Globerman also noted the problems were compounded by the US government’s low initial Medicare payments to private laboratories for COVID-19 tests. “Medicare is reputed to have paid about half the price it pays for a flu test, even though the coronavirus test is substantially more expensive to produce. The price forced labs to take losses on the test, blocking many labs from scaling up production to expand the nation’s testing capacity.
“Only after major lab organizations made public pleas for increased Medicare reimbursement, and long backlogs emerged for testing and reporting test results, did Medicare agree to double its payments for coronavirus tests,” Globerman wrote.
Could National Differences in Healthcare Systems Be to Blame for Disparate COVID-19 Outcomes?
In “Canada Succeeded on Coronavirus Where America Failed. Why?” Canadian public health experts told Vox differences in the two countries’ political leadership, public health funding, and healthcare systems are to blame for the US experiencing a worse coronavirus outbreak than Canada.
Is that true? Sally C. Pipes, CEO, and Thomas W. Smith Fellow in Health Care Policy at the Pacific Research Institute, a former resident of Canada and an ardent critic of single-payer healthcare, argued that Canada’s healthcare system is plagued by long waits for elective procedures, equipment shortages, and limited access to cutting-edge drugs and therapies.
In “The Canadian Health-Care Scare,” Pipes wrote, “Our northern neighbors wait months for routine care and lack access to the latest life-saving medications and technology. Importing this system would lead to widespread misery,” adding, “Is a six-month wait for a knee replacement—the median in Canada last year—reasonable, when it keeps someone in pain and unable to work? One study puts the total cost of waiting for joint-replacement surgery after taking into account lost wages and additional tests and scans at almost $20,000. It’s no wonder that more than 323,000 Canadians left the country to seek care abroad in 2017.”
A Fraser Institute study of wait times in Canada for medically-necessary treatments underscores Pipes’ claims. According to the study, the median wait time—from general practitioner referral to treatment—across 12 medical specialties was 20.9 weeks in 2019, the second highest recorded by the Institute. If this is the case, how did Canada earn praise for its early COVID-19 response?
It’s unclear what lessons American clinical laboratories can glean from Canada’s response to COVID-19. Nevertheless, lab managers should closely watch their counterparts in other nations around the world. The coronavirus does not respect borders or care about disparities in healthcare systems.
Multiple recent studies reveal a substantial number of patients continue to delay needed healthcare in the months since the onset of the SARS-CoV-2 outbreak
Based on an analysis of hospital emergency department (ED) usage, federal researchers concluded that patients continue to be cautious when visiting healthcare providers, including clinical laboratories, and that people are altering how they seek and utilize emergency care due to the COVID-19 pandemic. This not only reduces the number of typical test orders from the ER to the hospital lab, but also reduces the source of inpatient admissions.
Between March 29 and April 25 of this year, facilities the CDC examined recorded 1.2 million visits to EDs, compared to 2.1 million visits between March 31 and April 27 of last year. The steepest decrease in patient demographics was for individuals under the age of 14, women, and people living in the Northeast region.
The CDC’s data showed that 12% of ED visits were for children in pre-pandemic 2019, which dropped to 6% during the 2020 pandemic period. The CDC included ED visits from hospitals in 47 states (excluding Hawaii, South Dakota, and Wyoming) and captured information from approximately 73% of ED visits in the US.
Delaying Healthcare Visits Worsens Medical Conditions, Reduces Revenues
ED visits are an important referral source for inpatient admissions. Fewer patients in EDs means lost revenue for hospitals. However, one positive aspect of the waning number of ED visits is that it may be keeping patients with non-emergency situations away from emergency departments, thus reducing the overuse of costly ED visits. But healthcare professionals are concerned that individuals also may be avoiding or delaying care when needed, which could worsen medical situations and outcomes.
“We saw people, with COVID-19 and without, coming into the ED who were very ill,” Vik Reddy, MD, Chief Medical Officer at Wellstar Kennestone Hospital and Wellstar Windy Hill Hospital in the Atlanta area, told Modern Healthcare. He noted that some patients delayed care for critical non-COVID-19 illnesses. “The good news is that we’re seeing that trend reverse this time around. It was scary in March when we knew that people weren’t coming into the ED for heart attacks.”
The NSSP’s analysis concluded that the report’s findings were subject to at least four limitations:
The number of hospitals reporting to NSSP changes over time as facilities are added or closed. For example, 3,173 hospitals reported data in April of 2019, while 3,467 reported data in April 2020.
Diagnostic categories rely on the use of specific codes, which were missing in 20% of the ED visits reported.
NSSP coverage is not uniform across or within all the participating states.
The analysis is limited only to ED visits and does not take into account patients who did not go to an ED, but instead received treatment in other healthcare environments, such as urgent care clinics.
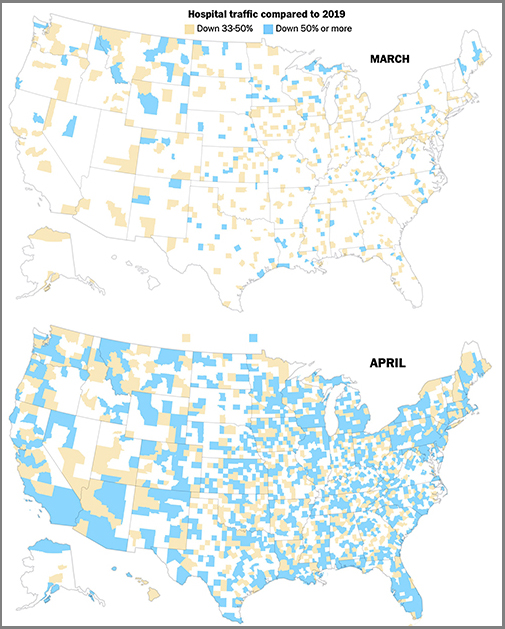
The graphics above are taken from a Washington Post article which reported that the newspaper’s analysis of smartphone location data of hospital traffic in 2020 showed the “drop” in hospital usage had turned into “a crash,” compared to the same two months last year, and that, “As in many other industries, those lost visits represented a widespread financial crisis for hospitals and other healthcare providers, even in places the novel coronavirus hardly touched.” (Graphics copyright: The Washington Post.)
Additional Studies Show Patients Avoiding Hospital EDs, Delaying Care
Other sources also are reporting similar findings regarding consumer attitudes towards seeking medical care during the COVID-19 pandemic. A PricewaterhouseCoopers survey released in May found that about 45% of 2,500 consumers surveyed plan to forgo their annual physical in 2020, due to the pandemic, Modern Healthcare reported.
In addition, an Optum Consumer Pulse Survey released in May found that nearly 20% of 700 surveyed individuals stated they were likely to avoid hospital EDs even if they were showing signs of a heart attack or appendicitis. Another 40% stated they were likely to avoid the ED if they had a cut that required stitches.
In “Americans Are Delaying Medical Care, and It’s Devastating Health-Care Providers,” The Washington Post analyzed hospital use during the pandemic based on smartphone tracking data. WaPo’s report found a significant drop in patients seeking in-person healthcare with many areas across the country reporting a 50% reduction in patients when compared to last year.
The article also states that almost 94 million people have delayed medical care due to the COVID-19 pandemic, and that 66 million of those individuals needed medical care unrelated to the virus but did not receive it.
These studies and others are showing a pattern. The COVID-19 pandemic has changed when and where patients access healthcare, and if the trend continues, it could have a long-term impact on clinical laboratories. Since fewer people are seeking medical care, fewer laboratory tests are being ordered and performed, which means less work and revenue for the nations’ hospital and independent clinical labs.
Australian government heralded April purchase of 10 million clinical laboratory diagnostics tests from BGI, but most of the nation’s states and territories say kits are unneeded or unable to be used by their health departments
While the United States and other nations attempt to bring the COVID-19 outbreak under control, many countries have turned to China to offset shortages of clinical laboratory SARS-CoV-2 test kits needed to diagnose the coronavirus. This did not work out well for the United Kingdom and Spain, each which purchased large volumes of COVID-19 test kits from Chinese companies in April.
Now comes news that Australia spent roughly $130 million US ($200 million AUD) in late April for COVID-19 RT-PCR tests from BGI Genomics. However, those kits are mainly going unused as Australian state governments say they are unneeded or incompatible with existing testing equipment.
This is the latest example of the problems plaguing governments worldwide as they scramble to boost SARS-CoV-2 testing capacity during the evolving pandemic.
The new problem is that COVID-19 testing capacity has increased so much it now exceeds demand for testing. This is true for portions of Australia and in some states in the US.
Demand for Testing in Australia Far Lower than Expected
With a population of roughly 25 million, Australia has a smaller population than Texas, which in 2020 stood at about 28 million. According to the Johns Hopkins COVID-19 Dashboard, Australia had 7,139 confirmed cases of COVID-19 as of May 27 and 103 deaths.
Australian billionaire Andrew “Twiggy” Forrest, former CEO of Fortescue Metals Group, orchestrated the purchase of 10 million COVID-19 RT-PCR testing kits for Australia from BGI. He did so through his philanthropic organization, the Minderoo Foundation, with the understanding that the purchase cost would be refunded by the Australian government.
On April 28, the Australian government heralded Forrest’s purchase as a commercial coup, because it occurred in the midst of sparring between the two countries over China’s handling of the coronavirus outbreak and fierce international competition for COVID-19 diagnostic testing kits.
“Today we are securing perhaps the most critical step in our testing capability,” Australia’s Minister for Health Greg Hunt, MP (above) stated during a press conference, reported ABC News. “What these 10 million tests will do is allow our state and territory public health units to be able to test right through 2020. [They] provide us with the capacity to contain, suppress and defeat the virus, but also if a case were to emerge, to find it and to find everybody around.” However, demand for testing has not been as great as Australia’s leaders had anticipated. (Photo copyright: ABC News.)
Forrest credited his personal relationship with BGI for his ability to secure the kits for Australia. “Chairman Wang [Jian] and BGI kept to their word and resisted that very clear temptation of a businessman to make a much bigger profit and maintain the integrity of my relationship, and I’m very grateful for that,” Forrest told ABC News.
However, less than a month later, The Guardian Australia reported the taxpayer-funded coronavirus testing kits Forrest brought to Australia were not being used. Instead, the test kits have been added to the country’s strategic reserve. Three of five Australian states and both territories—Queensland, New South Wales, Western Australia, the Northern Territory, and the Australian Capital Territory—all told the newspaper they were not using the BGI tests. Only Victoria reported it was using the BGI tests.
“PathWest, Western Australia’s leading pathology laboratory, is not using the BGI-manufactured COVID-19 PCR testing kits,” the Western Australia Department of Health told The Guardian. “PathWest has capacity and sufficient reagent to provide testing throughout the state without the need to use these tests.”
“Queensland Health does not use the BGI COVID-19 test or its operating platform,” a spokeswoman told The Guardian. “Queensland already has ample testing capacity, illustrated by the world leading figures of 137,000 COVID-19 tests since January.”
According to ABC News, Minderoo also purchased 11 testing machines, which were installed around the country. Six Chinese experts flew to Australia to help oversee the testing machines’ installation.
Testing Capacity Also Exceeds Demand in US
Increased COVID-19 testing capacity has been considered a cornerstone to fully lifting stay-at-home orders and reopening businesses, schools, and entertainment venues. But Australia is not alone in ramping up testing capacity only to have public demand not keep pace. The Washington Post reported in mid-May that in at least a dozen states COVID-19 testing capacity exceeded the number of patients lining up for testing.
Utah Department of Health spokesperson Tom Hudachko is among those questioning why people aren’t getting tested in his state, which has a 9,000-test capacity, but was conducting only 3,500 tests a day.
“Well, that’s the million-dollar question,” Hudachko told the Washington Post. “It could be simply that people don’t want to be tested. It could be that people feel like they don’t need to be tested. It could be that people are so mildly symptomatic that they’re just not concerned that having a positive lab result would actually change their course in any meaningful way.”
Meanwhile, Australia’s federal government has the interesting problem of having purchased $130 million (US) of COVID-19 test kits from a Chinese company—test kits that most of the nation’s states and territories have yet to use. Could this be a sign that many clinical laboratory scientists in Australia have their doubts about the accuracy and reliability of these Chinese-manufactured COVID-19 tests?
Washington Post investigation outlines scientists’ frustrations in the early days of the pandemic, as they worked to deploy laboratory-developed tests for the novel coronavirus
In the wake of the failed rollout of the Centers for Disease Control and Prevention’s (CDC) COVID-19 diagnostic test last February, many CLIA-certified academic and public health laboratories were ready, and had the necessary resources, to develop their own coronavirus molecular diagnostic tests to help meet the nationwide demand for clinical laboratory testing. However, the response from the US Food and Drug Administration (FDA) was, in essence, “not so fast.”
In this second part of Dark Daily’s two-part e-briefing, we continue our coverage of the Washington Post (WP) investigation that detailed the regulatory hurdles which blocked private laboratories from deploying their own laboratory-developed tests (LDTs) for COVID-19. The report is based on previously unreported email messages and other documents reviewed by the WP, as well as the newspaper’s exclusive interviews with scientists and officials involved.
The CDC’s COVID-19 test kits began arriving at public health laboratories on February 8, just 18 days after the first case of the novel coronavirus was confirmed in the US. As the WP noted in an earlier analysis, titled, “What Went Wrong with Coronavirus Testing in the US,” the CDC’s decision to develop its own test was not surprising. “The CDC will develop [its] own test that is suited to an American healthcare context and the regulations that exist here,” explained Jeremy Konyndyk, Senior Policy Fellow at the Center for Global Development. “That’s how we normally would do things.”
But state and local public health laboratories quickly discovered that the CDC test kits were flawed due to problems with one of the reagents. While numerous academic, research, and commercial labs had the capability to produce their own COVID-19 PCR tests, FDA rules initially prevented them from doing so without a federal Emergency Use Authorization (EUA).
The bureaucratic hurdles arose due to Health and Human Services Secretary Alex Azar’s January 31 declaration that COVID-19 was a “health emergency” in the US. By doing so, HHS triggered a mandate that requires CLIA-certified labs at universities, research centers, and hospitals to seek an EUA from the FDA before deploying any laboratory-developed tests.
Scientists, Clinical Laboratories Frustrated by Bureaucratic Delays and Red Tape
To make matters worse, the EUA process was neither simple nor fast, which exasperated lab scientists and clinical laboratory administrators. “In their private communications, scientists at academic, hospital, and public health labs—one layer removed from federal agency operations—expressed dismay at the failure to move more quickly, and frustration at bureaucratic demands that delayed their attempts to develop alternatives to the CDC test,” wrote the WP investigators.
In a Feb. 27 email to other microbiologists, Marc Couturier, PhD, Medical Director at ARUP Laboratories, a national reference laboratory network located in Utah, voiced his irritation with the red tape that stymied private laboratory development of COVID-19 tests. He wrote, “We have the skills and resources as a community, but we are collectively paralyzed by a bloated bureaucratic/administrative process,” reported the WP.
Keith Jerome, MD, PhD (above), Head of the Virology Division at the Fred Hutchinson Cancer Research Center in Seattle, maintains federal regulations muted one of the nation’s greatest assets in the fight against COVID-19. “The great strength the US has always had, not just in virology, is that we’ve always had a wide variety of people and groups working on any given problem,” he told MIT Technology Review. “When we decided all coronavirus testing had to be done by a single entity, even one as outstanding as CDC, we basically gave away our greatest strength.” (Photo copyright: Jonathan Hamilton/NPR.)
‘FDA Should Not Treat Labs Like They Are Creating Commercial Products’
According to Kaiser Health News (KHN), Greninger was able to identify one of the nation’s first cases of community-acquired COVID-19 by taking “advantage of a regulatory loophole that allowed the lab to test samples obtained for research purposes from UW’s hospitals.”
But navigating the EUA process was a different story, Greninger told the WP. He spent more than 100 hours filling out forms and collecting information needed for the EUA application. After emailing the application to the FDA, Greninger received a reply containing eCopy Guidance telling him he needed to resubmit the information to the Document Control Center (DCC) at the Center for Devices and Radiological Health (CDRH), a federal agency Greninger knew nothing about. Another FDA rule required that the submission be copied to a hard disk and mailed to the DCC.
In an interview with ProPublica, Greninger stated that after he submitted his COVID-19 test—which copies the CDC protocol—an FDA reviewer told him he would need to prove the test would not show a positive result for someone infected with either a SARS or MERS coronavirus. The first SARS coronavirus disappeared in mid-2003 and the only two cases of MERS in the US were diagnosed in 2014. Greninger told ProPublica it took him two days to locate a clinical laboratory that could provide the materials he needed.
Greninger maintains the FDA should not treat all clinical laboratories as though they are making a commercial product. “I think it makes sense to have this regulation when you’re going to sell 100,000 widgets across the US. That’s not who we are,” he told ProPublica.
FDA Changes Course
Under pressure from clinical laboratory scientists and medical doctors, by the end of February the FDA had issued new policy that enabled CLIA-certified laboratories to immediately use their validated COVID-19 diagnostics while awaiting an EUA. “This policy change was an unprecedented action to expand access to testing,” said the FDA in a statement.
Since then, the FDA has continued to respond—albeit slowly—to scientists’ complaints about regulations that hampered the nation’s COVID-19 testing capacity.
Clinical laboratory leaders and pathologists involved in testing for the SARS-CoV-2 coronavirus should monitor the FDA’s actions and be aware of when and if certain temporary changes the agency implemented during the early days of the COVID-19 pandemic become permanent.
To read part one of our two-part coverage of the Washington Post’s investigation, click here.
Previously unreported email messages and documents paint vivid picture of public health laboratory officials’ dismay and frustration over testing delays
Between late January and early March, Clinical laboratory leaders watched with dismay as federal government missteps crippled the Centers for Disease Control and Prevention’s (CDC) rollout of its COVID-19 diagnostic testing in the early days of the pandemic. The resulting lack of testing capacity enabled the novel coronavirus’ spread across the United States.
This first part of Dark Daily’s two-part e-briefing covers how investigators at the Washington Post (WP) have produced a timeline describing the CDC initial failure to produce a reliable laboratory test for COVID-19 and the regulatory hurdles that blocked medical laboratories from developing their own tests for the virus. The WP’s report is based on previously unreleased email messages and other documents reviewed by the WP, as well as the newspaper’s exclusive interviews with medical laboratory scientists and officials involved.
A New York Times report on the federal government’s initial review of the testing kit failure pinned the blame on sloppy practices at CDC laboratories in Atlanta and a lack of expertise in commercial manufacturing. However, the WP reported that COVID-19 testing kits were delayed due to a “glaring scientific breakdown” at the central lab, created when the CDC facilities that assembled the kits “violated sound manufacturing practices” that resulted in cross contamination of testing compounds.
The US and other countries have criticized China for a lack of transparency about the virus’ emergence, which came to light on December 31, 2019, when China reported a cluster of pneumonia cases in Wuhan, according to a World Health Organization (WHO) timeline. A week later, Chinese authorities identified the pneumonia-like illness as being caused by a new novel coronavirus.
In the US, the first case of COVID-19 was found January 21 in a Washington State man who had traveled to Wuhan. But in the weeks that followed, the US government’s inability to establish a systematic testing policy became the catalyst for the virus’ ultimate spread to more than two million people, notes the CDC website.
ProPublica, which conducted its own investigation into the early stages of the government’s coronavirus response, blamed the failures on “chaos” at the CDC and “an antiquated public health system trying to adapt on the fly.”
The CDC’s first mistake may have been underestimating the danger COVID-19 posed to public health in this country. During a January 15 conference call, CDC scientists assured state and county public health officials that the agency was developing a COVID-19 diagnostic test which soon would be available, but which may not be needed “unless the scope gets much larger than we anticipate right now,” reported the WP.
A week later, an interview with CNBC, President Trump said, “We have it under control. It’s going to be just fine.”
CDC scientists designed their test in seven days, which, according to the WP investigators, is “a stunningly short period of time for a healthcare system built around the principles of medical quality and patient safety, not speed.” But when those initial CDC-made tests arrived at a New York City public health laboratory on February 8, lab technicians discovered the COVID-19 assays often indicated the presence of the coronavirus in samples that the lab’s scientists knew did not contain the virus.
When the scientists informed Lab Director Jennifer Rakeman, PhD, Assistant Commissioner, New York City Department of Health and Mental Hygiene, her response, according to the WP, was “Oh, s—. What are we going to do now?”
That night, Director Jill Taylor, PhD, Director of New York State’s Wadsworth Center public health reference laboratory, emailed state health officials, stating, “There is a technical problem in one of the reagents which invalidates the assay and will not allow us to perform the assay,” reported the WP. “I’m sorry not to have better news.”
Scott Becker (above), Executive Director of the Association of Public Health Laboratories (APHL), voiced his concerns about the CDC’s flawed COVID-19 test kits in an email to a CDC official, reported the WP. “The states and their governors are going to come unglued,” Becker wrote, adding, “If the CDC doesn’t get ahead of this, it will be a disaster.” (Photo copyright: Bill O’Leary/The Washington Post.)
‘The Silence from CDC is Deafening’
On February 10, Joanne Bartkus, PhD, then-Lab Director of the Minnesota Health of Department, wrote to APHL Executive Director Scott Becker: “The silence from CDC … is deafening. What is going on?” reported the WP.
By the end of February, the Associated Press (AP) reported that only 472 patients had been tested for COVID-19 nationwide. By comparison, South Korea, which identified its first case of COVID-19 on the same day as the US, was testing 1,000 people per day.
A WHO spokesperson told the WP that, “… no discussions occurred between WHO and CDC (or other US government agencies) about WHO providing COVID-19 tests to the US.” When the CDC’s original COVID-19 test kit failed, there may not have been a Plan B. This may explain why the opportunity to contain COVID-19 through surveillance testing was lost during the weeks it took to design a fix for the CDC test and loosen regulations so clinical laboratories could develop their own tests.
As medical laboratory scientists and clinical laboratory leaders know, the lack of early COVID-19 testing was a public health failure and painted a false picture of the virus’ spread. Nearly five months after the first case of the virus was confirmed in the US, testing capacity may only now be outpacing demand.
Click here to read part two of our coverage of the Washington Post’s investigation.