Another study in the United Kingdom that also used genomic analysis to understand drug-resistant Shigella produced findings that may be useful for microbiologists and medical laboratory scientists
From the onset of an infectious disease outbreak, public health officials, microbiologists, and clinical laboratory managers find it valuable to trace the origin of the spread back to the “index case” or “patient zero”—the first documented patient in the disease epidemic. Given the decreased cost of genomic analysis and improved accuracy of gene sequencing, infectious disease researchers are finding that task easier and faster than ever.
One recent example is a genomic study conducted at University of Washington (UW) in Seattle that enabled researchers to “retrace” the origin and spread of a “multidrug-resistant Shigellosis outbreak” from 2017 to 2022. “The aim of the study was to better understand the community transmission of Shigella and spread of antimicrobial resistance in our population, and to treat these multi-drug resistant infections more effectively,” the UW scientists stated in a new release.
Shigellosis (aka, bacillary dysentery) is a highly contagious disease of the intestines that can lead to hospitalization. Symptoms include fever, stomach cramps, diarrhea, dysentery, and dehydration.
“Additional analysis of the gut pathogen and its transmission patterns helped direct approaches to testing, treatment, and public health responses,” the UW news release states.
Usually prevalent in countries with public health and sanitation limitations, the “opportunistic” Shigella pathogen is now being seen in high-income countries as well, UW reported.
“You can’t really expect an infectious disease to remain confined to a specific at-risk population. [Shigella infections are] very much an emerging threat and something where our public health tools and therapeutic tools have significant limitations,” infectious disease specialist Ferric Fang, MD (above) told CIDRAP News. Fang is a UW professor of Microbiology and Clinical Laboratory Medicine and a corresponding author of the UW study. (Photo copyright: University of Washington.)
Generally, Shigella infects children, travelers, and men who have sex with men (MSM), the CDC noted.
The UW researchers were motivated to study Shigella when they noticed an uptick in drug-resistant shigellosis cases in Seattle’s homeless population in 2020 at the beginning of the COVID-19 pandemic, Center for Infectious Disease Research and Policy News (CIDRAP News) reported.
“Especially during the pandemic, a lot of public facilities were closed that homeless people were used to using,” infectious disease specialist Ferric Fang, MD, told CIDRAP News. Fang is Professor of Microbiology and Laboratory Medicine at University of Washington and corresponding author of the UW study.
The researchers studied 171 cases of Shigella identified from 2017 to 2022 by clinical laboratories at Harborview Medical Center and UW Medical Center in Seattle. According to CIDRAP News, the UW researchers found that:
46% were men who have sex with men (MSM).
51% were people experiencing homelessness (PEH).
Fifty-six patients were admitted to the hospital, with eight to an intensive care unit.
51% of isolates were multi-drug resistant (MDR).
Whole-Genome Sequencing Reveals Origin
The UW scientists characterized the stool samples of Shigella isolates by species identification, phenotypic susceptibility testing, and whole-genome sequencing, according to their Lancet Infectious Diseases paper. The paper also noted that 143 patients received antimicrobial therapy, and 70% of them benefited from the treatment for the Shigella infection.
Whole-genome sequencing revealed that two strains of Shigella (S. flexneri and S. sonnei) appeared first in Seattle’s MSM population before infecting the PEM population.
The genomic analysis found the outbreak of drug-resistant Shigella had international links as well, according to CIDRAP News:
One S. flexneri isolate was associated with a multi-drug resistant (MDR) strain from China, and
S. sonnei isolates resembled a strain characteristic of a current outbreak of MDR Shigella in England.
“The most prevalent lineage in Seattle was probably introduced to Washington State via international travel, with subsequent domestic transmission between at-risk groups,” the researchers wrote.
“Genomic analysis elucidated not only outbreak origin, but directed optimal approaches to testing, treatment, and public health response. Rapid diagnostics combined with detailed knowledge of local epidemiology can enable high rates of appropriate empirical therapy even in multidrug-resistant infection,” they continued.
UK Shigella Study Also Uses Genomics
Another study based in the United Kingdom (UK) used genomic analysis to investigate a Shigella outbreak as well.
Motivated by a UK Health Security Agency report of an increase in drug-resistance to common strains since 2021, the UK researchers studied Shigella cases from September 2015 to June 2022.
According to a paper they published in Lancet Infectious Diseases, the UK researchers “reported an increase in cases of sexually transmitted S. flexneri harboring blaCTX-M-27 (an antibiotic-resistant gene) in England, which is known to confer resistance to third-generation cephalosporins (antibiotics),” the researchers wrote.
Their analysis of plasmids (DNA with genes having antibiotic resistance) revealed a link in two drug-resistant Shigella strains at the same time, CIDRAP News explained.
“Our study reveals a worsening outlook regarding antimicrobial-resistant Shigella strains among MSM and highlights the value of continued integration of genomic analysis into surveillance and research,” the UK-based scientists wrote.
Current challenges associated with Shigella, especially as it evades treatment, may continue to demand attention from microbiologists, clinical laboratory scientists, and infectious disease specialists. Fortunately, use of genomic analysis—due to its ongoing improvements that have lowered cost and improved accuracy—has made it possible for public health researchers to better track the origins of disease outbreak and spread.
CDC advises clinical laboratories and microbiologists encountering C. auris to follow their own protocols before adopting federal agency guidelines
In July, the Centers for Disease Control and Prevention (CDC) warned healthcare facilities and clinical laboratories to be on the alert for Candida auris (C. auris) infections in their patients. An outbreak of the drug resistant and potentially deadly fungus had appeared in two Dallas hospitals and a Washington D.C. nursing home.
Since those outbreaks, researchers have studied with urgency the “superbug’s” emergence in various types of healthcare facilities around the nation, not just hospitals. Their goal was to discover how it was successfully identified and contained.
“Seeing what was happening in New York, New Jersey, and Illinois [was] pretty alarming for a lot of the health officials in California [who] know that LTACHs are high-risk facilities because they take care of [very] sick people. Some of those people are there for a very long time,” the study’s lead author Ellora Karmarkar, MD, MSc, told Medscape. Karmarkar is an infectious disease fellow with the University of Washington and formerly an epidemic intelligence service officer with the CDC.
“One of the challenges was that people were so focused on COVID that they forgot about the MDROs (multi-drug resistant organisms] … Some of the things that we recommend to help control Candida auris are also excellent practices for every other organism including COVID care,” she added.
According to Medscape, “The OCHD researchers screened LTACH and vSNF patients with composite cultures from the axilla-groin or nasal swabs. Screening was undertaken because 5%–10% of colonized patients later develop invasive infections, and 30%–60% die.
Medscape also reported that the first bloodstream infection was detected in May 2019, and that, according to the Annals of Internal Medicine study, as of January 1, 2020, of 182 patients:
22 (12%) died within 30 days of C. auris identification,
“This is really the first time we’ve seen clustering of resistance in which patients seemed to be getting the infections from each other,” Meghan Lyman, MD, Medical Officer in the Mycotic Diseases Branch of the CDC, told Fox News.
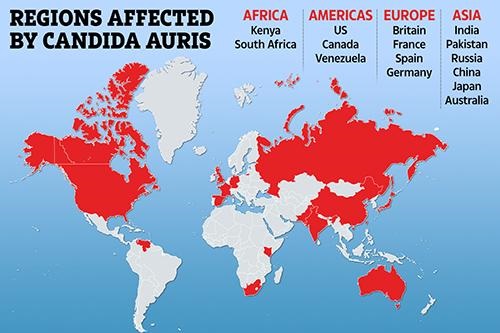
The graphic above illustrates how Candida auris is “spanning the globe,” The New York Times reported. Clinical laboratories that encounter this potentially deadly fungus are advised to contact the CDC immediately for guidance and to take proactive steps to prepare for the “superbug’s” arrival. (Graphic copyright: The Scottish Sun.)
Be More Proactive than Reactive in Identifying C. Auris, CDC Says
C. auris is a type of yeast infection that can enter the bloodstream, spread throughout the body, and cause serious complications. People who appear to have the highest risk of contracting the infection are those:
Who have had a lengthy stay in a healthcare facility,
Individuals connected to a central venous catheter or other medical tubes, such as breathing or feeding tubes, or
Have previously received antibiotics or antifungal medications.
It tends to be resistant to the antifungal drugs that are commonly used to treat Candida infections.
It can be difficult to identify via standard laboratory testing and is easily misidentified in labs without specific technology.
It can quickly lead to outbreaks in healthcare settings.
“With all this spread that we’ve been seeing across the country we’re really encouraging health departments and facilities to be more proactive instead of reactive to identifying Candida auris in general,” Lyman told STAT. “Because we’ve found that controlling the situation and containing spread is really easiest when it’s identified early before there’s widespread transmission.”
There continues to be concerns over this highly drug-resistant infection among hospital physicians and medical laboratories. “Acute care hospitals really ought to be moving toward doing species identification of Candida from nonsterile sites if they really want to have a better chance of detecting this early,” Dan Diekema, MD (above), an epidemiologist and clinical microbiologist at the University of Iowa, told Medscape. (Photo copyright: University of Iowa.)
Candia Auris versus Other Candida Infections
C. auris can cause dangerous infections in the bloodstream and spread to the central nervous system, kidneys, liver, spleen, bones, muscles, and joints. It spreads mostly in long-term healthcare facilities among patients with other medical conditions.
The symptoms of having a Candida auris infection include:
Fever
Chills
Pain
Redness and swelling
Fluid drainage (if an incision or wound is present)
General feeling of tiredness and malaise
C. auris infections are typically diagnosed via cultures of blood or other bodily fluids, but they are difficult to distinguish from more common types of Candida infections, and special clinical laboratory tests are needed to definitively diagnose C. auris.
Whole-genome Sequencing of C. Auris and Drug Resistance
The CDC conducted whole-genome sequencing of C. auris specimens gathered in Asia, Africa, and South America and discovered four different strains of the potentially life-threatening Candida species. All four detected strains have been found in the United States.
There are only three classes of antifungal drugs used to treat Candida auris infections:
However, 85% of the infections in the US have proven to be resistant to azoles and 38% are resistant to polyenes. Patients respond well to echinocandins, but more effective therapies are needed especially as some isolates may become resistant while a patient is on drug therapy, STAT reported.
“Even while it might be susceptible upfront, after a week or two of therapy, we may find that the patient has an infection now caused by an isolate of the same Candida auris that has become resistant to the echinocandins and we are really left with nothing else,” Jeffrey Rybak, PhD, PharmD, Instructor, Department of Pharmaceutical Sciences, St. Jude Children’s Research Hospital, told Infection Control Today.
Although relatively rare, C. auris infections are on the rise. The good news is that there may be further pharmaceutical help available soon. New antifungal agents, such as Ibrexafungerp (Brexafemme) show promise in fighting C. auris infections, but more research is needed to prove their efficacy.
What Should Clinical Laboratories Do?
The CDC stresses that clinical laboratories and microbiologists working with known or suspected cases of Candida auris should first adhere to their own safety procedures. The CDC issued guidelines, but they are not meant to supersede the policies of individual labs.
The CDC also recommends that healthcare facilities and clinical laboratories that suspect they have a patient with a Candida auris infection immediately contact the CDC and state or local public health authorities for guidance.
With improved genetic sequencing comes larger human genome databases that could lead to new diagnostic and therapeutic biomarkers for clinical laboratories
As the COVID-19 pandemic grabbed headlines, the human genome database at the US Department of Veterans Affairs Million Veterans Program (MVP) quietly grew. Now, this wealth of genomic information—as well as data from other large-scale genomic and genetic collections—is expected to produce new biomarkers for clinical laboratory diagnostics and testing.
In December, cancer genomics company Personalis, Inc. (NASDAQ:PSNL) of Menlo Park, Calif., achieved a milestone and delivered its 100,000th whole human genome sequence to the MVP, according to a news release, which also states that Personalis is the sole sequencing provider to the MVP.
The VA’s MVP program, which started in 2011, has 850,000 enrolled veterans and is expected to eventually involve two million people. The VA’s aim is to explore the role genes, lifestyle, and military experience play in health and human illness, notes the VA’s MVP website.
Health conditions affecting veterans the MVP is researching include:
The VA has contracted with Personalis through September 2021, and has invested $175 million, Clinical OMICS reported. Personalis has earned approximately $14 million from the VA. That’s about 76% of the company’s revenue, according to 2nd quarter data, Clinical OMICS noted.
“The VA MVP is the largest whole genome sequencing project in the United States, and this is a significant milestone for both the program and for Personalis,” said John West (above with wife Judy), Founder and CEO of Personalis, in the news release. “Population-scale sequencing projects of this nature represent a cornerstone in our effort to accelerate the advancement of precision medicine across a wide range of disease areas,” he added. (Photo copyright: MIT Technology Review.)
Database of Veterans’ Genomes Used in Current Research
What has the VA gained from their investment so far? An MVP fact sheet states researchers are tapping MVP data for these and other veteran health-related studies:
Differentiating between prostate cancer tumors that require treatment and others that are slow-growing and not life-threatening.
How genetics drives obesity, diabetes, and heart disease.
How data in DNA translates into actual physiological changes within the body.
Gene variations and patients’ response to Warfarin.
NIH Research Program Studies Effects of Genetics on Health
Another research program, the National Institutes of Health’s All of Us study, recently began returning results to its participants who provided blood, urine, and/or saliva samples. The NIH aims to aid research into health outcomes influenced by genetics, environment, and lifestyle, explained a news release. The program, launched in 2018, has biological samples from more than 270,000 people with a goal of one million participants.
“We’re changing the paradigm for research. Participants are our most important partners in this effort, and we know many of them are eager to get their genetic results and learn about the science they’re making possible,” said Josh Denny, MD, CEO of the NIH’s All of Us research program in the news release. Denny, a physician scientist, was Professor of Biomedical Informatics and Medicine, Director of the Center for Precision Medicine and Vice President for Personalized Medicine at Vanderbilt University Medical Center prior to joining the NIH. (Photo copyright: National Institutes of Health.)
Inclusive Data Could Aid Precision Medicine
The news release notes that more than 80% of biological samples in the All of Us database come from people in communities that have been under-represented in biomedical research.
“We need programs like All of Us to build diverse datasets so that research findings ultimately benefit everyone,” said Brad Ozenberger, PhD, All of Us Genomics Program Director, in the news release.
Precision medicine designed for specific healthcare populations is a goal of the All of Us program.
“[All of Us is] beneficial to all Americans, but actually beneficial to the African American race because a lot of research and a lot of medicines that we are taking advantage of today, [African Americans] were not part of the research,” Chris Crawford, All of US Research Study Navigator, told the Birmingham Times. “As [the All of Us study] goes forward and we get a big diverse group of people, it will help as far as making medicine and treatment that will be more precise for us,” he added.
Large Databases Could Advance Care
Genome sequencing technology continues to improve. It is faster, less complicated, and cheaper to sequence a whole human genome than ever before. And the resulting sequence is more accurate.
Thus, as human genome sequencing databases grow, researchers are deriving useful scientific insights from the data. This is relevant for clinical laboratories because the new insights from studying bigger databases of genomic information will produce new diagnostic and therapeutic biomarkers that can be the basis for new clinical laboratory tests as well as useful diagnostic assays for anatomic pathologists.
Low prices to encourage consumers to order its WGS service is one way Veritas co-founder and genetics pioneer George Church hopes to sequence 150,000 genomes by 2021
By announcing an annotated whole-genome sequencing (WGS) service to consumers for just $599, Veritas Genetics is establishing a new price benchmark for medical laboratories and gene testing companies. Prior to this announcement in July, Veritas priced its standard myGenome service at $999.
“There is no more comprehensive genetic test than your whole genome,” Rodrigo Martinez, Veritas’ Chief Marketing and Design Officer, told CNBC. “So, this is a clear signal that the whole genome is basically going to replace all other genetic tests. And this [price drop] gets it closer and closer and closer.”
Pathologists and clinical laboratory managers will want to watch to see if Veritas’ low-priced, $599 whole-genome sequencing becomes a pricing standard for the genetic testing industry. Meanwhile, the new price includes not only the sequencing, but also an expert analysis of test results that includes information on more than 200 conditions, Veritas says.
“The focus in our industry is shifting from the cost of sequencing genomes to interpretation capabilities and that’s where our secret sauce is,” said Veritas CEO Mirza Cifric in a news release. “We’ve built and deployed a world class platform to deliver clinically-actionable insights at scale.” The company also says it “achieved this milestone primarily by deploying internally-developed machine learning and AI [artificial intelligence] tools as well as external tools—including Google’s DeepVariant—and by improving its in-house lab operations.”
The myGenome service offers 30x WGS, which Veritas touts in company documentation as the “gold standard” for sequencing, compared to the less-precise 0.4x WGS.
The myGenome service is available only in the United States.
Will Whole-Genome Sequencing Replace Other Genetic Tests?
Veritas was co-founded by George Church, PhD, a pioneer of personal genomics through his involvement with the Harvard Personal Genome Project at Harvard Medical School. In a press release announcing the launch of myGenome in 2016, Veritas described its system as “the world’s first whole genome for less than $1,000, including interpretation and genetic counseling.”
Church predicts that WGS will someday replace other genetic tests, such as the genotyping used by personal genomics and biotechnology company 23andMe.
“Companies like 23andMe that are based on genotyping technology basically opened the market over the last decade,” Martinez explained in an interview with WTF Health. “They’ve done an incredible job of getting awareness in the general population.”
However, he goes on to say, “In genotyping technology, you
are looking at very specific points of the genome, less than half of one
percent, a very small amount.”
Martinez says Veritas is sequencing all 6.4 billion letters
of the genome. And, with the new price point, “we’re closer to realizing that
seismic shift,” he said in the news release.
“This is the inflection point,” Martinez told CNBC.
“This is the point where the curve turns upward. You reach a critical mass when
you are able to provide a product that gives value at a specific price point.
This is the beginning of that. That’s why it’s seismic.”
Rodrigo Martinez (above), Veritas’ Chief Marketing and Design Officer, told CNBC, “The only way we’re going to be able to truly extract the value of the genome for a healthier society is going to be analyzing millions of genomes that have been sequenced. And the only way we can get there is by reducing the price so that more consumers can sequence their genome.” Photo copyright: Twitter.)
Payment Models Not Yet Established by Government, Private
Payers
However, tying WGS into personalized medicine that leads to actionable diagnoses may not be easy. Robin Bennett, PhD (hon.), a board certified senior genetic counselor and Professor of Medicine and Medical Genetics at UW School of Medicine, told CNBC, “[Healthcare] may be moving in that direction, but the payment for testing and for services, it hasn’t moved in the preventive direction. So, unless the healthcare system changes, these tests may not be as useful because … the healthcare system hasn’t caught up to say, ‘Yes, we support payment for this.’”
“Insurers are looking for things where, if you get the
information, there’s something you can do with it and that both the provider
and the patient are willing and able to use that information to do things that
improve their health,” Phillips told CNBC. “Insurers are very interested
in using genetic testing for prevention, but we need to . . . demonstrate that
the information will be used and that it’s a good trade-off between the
benefits and the costs.”
Sequencing for Free If You Share Your Data
Church may have an answer for that as well—get biopharmaceutical companies to foot the bill. Though Veritas’ new price for their myGenome service is significantly lower than before, it’s not free. That’s what Nebula Genomics, a start-up genetics company in Massachusetts co-founded by Church, offers people willing to share the data derived from their sequencing. To help biomedical researchers gather data for their studies, Nebula provides free or partially-paid-for whole-genome sequencing to qualified candidates.
“Nebula will enable individuals to get sequenced at much
lower cost through sequencing subsidies paid by the biopharma industry,” Church
told BioSpace.
“We need to bring the costs of personal genome sequencing close to zero to
achieve mass adoption.”
So, will lower-priced whole-genome sequencing catch on?
Perhaps. It’s certainly popular with everyday people who want to learn their
ancestry or predisposition to certain diseases. How it will ultimately affect
clinical laboratories and pathologists remains to be seen, but one thing is
certain—WGS is here to stay.
The resulting genomic dataset may provide useful diagnostic insights that can be used by clinical laboratory and pathology professionals to learn how and why some people age with good health
Why do some seniors age in good health and other seniors
suffer with multiple chronic conditions? A new genetic database is using whole-genomic
sequencing (WGS) to answer that question in ways that may benefit medical
laboratories.
Because of the rapid aging of populations in the United
States and other developed nations throughout the world, there is keen interest
in how to keep seniors healthy. In fact, developing effective lab testing
services in support of improved senior health is one of the big opportunities
for both clinical laboratories and anatomic
pathology groups.
Until recent years, most clinical
pathologists dealt primarily with lab tests that used specimens such as blood
and urine. However, genetics researchers are using WGS to discover new causes
for many chronic illnesses. And the tools these researchers are developing offer
pathologists and clinical
laboratories powerful new ways to help doctors diagnose disease.
Through the use of WGS, the MGRB now features a huge
database of thousands of healthy elderly people. The data it contains may enable
pathology scientists to learn, from a genetic standpoint, why some people age
healthfully while others do not.
The researchers published their work titled, “The Medical
Genome Reference Bank: A Whole-Genome Data Resource of 4,000 Healthy Elderly
Individuals. Rationale and Cohort Design,” in the European Journal of
Human Genetics.
Finding New Applications for Genetic Data
According to the UNSW published study, “The MGRB is comprised
of individuals consented through the biobank programs of two contributing
studies … Each sample is from an individual who has lived to [greater than or
equal to] 70 years with no reported history or current diagnosis of
cardiovascular disease, dementia, or cancer, as confirmed by the participating
studies at recent follow-up study visits.”
The researchers noted in their paper, “Aged and healthy
populations are more likely to be selectively depleted of pathogenic alleles, and therefore
particularly suitable as a reference population for the major diseases of
clinical and public health importance.”
The MGRB plans to make its database openly accessible to the
international research community through its website once all 4,000 samples
have been sequenced. Currently, about 3,000 of the samples have been analyzed,
as noted on the Garvan website,
which is tracking the MGRB’s progress.
“The Medical Genome Reference Bank can tell us much about what it means to grow old but remain well, and is a powerful tool to help us deconstruct the genetics of common diseases,” said David Thomas, PhD (above), an NHMRC Principal Research Fellow, Director of The Kinghorn Cancer Center, and Head of the Cancer Division of the Garvan Institute in New South Wales, AU, in a statement reported by GenomeWeb. (Photo copyright: South West Sydney Research.)
Personal Genetic Data in Precision Medicine
“The integration of genomic knowledge and technologies into
healthcare is revolutionizing the way we approach clinical and public health
practice,” Caron
M. Molster, et al, noted in, “The Evolution of Public Health
Genomics: Exploring Its Past, Present, and Future,” published in Frontiers
in Public Health. Molster is Manager at the Health Department Western
Australia in Perth, and lead author of the paper.
“Public health genomics has evolved to responsibly integrate
advancements in genomics into the fields of personalized
medicine and public health,” the researchers wrote.
The 100,000
Genomes Project in the United Kingdom is sequencing the genomes of people
who have rare diseases and their families. Researchers all over the world are collecting
genomic data with plans to use it in different ways, and on various chronic
disease populations, in pursuit of precision medicine
goals.
Molster and her co-authors noted the comparable development
of genetic sequencing and precision medicine in their paper.
“Parallel to the developments in precision medicine has been
the advancement of technologies that enable the production, aggregation,
analysis, and dissemination of extremely large volumes of individual- and
population-level data on genes, environment, behavior, and other social and
economic determinants of health. These data have proven useful in finding new
correlations, patterns and trends, particularly those involving complex
interactions, in relation to diseases, pathogens, exposures, behaviors,
susceptibility (risk), and health outcomes in populations,” they wrote.
According to Paul Lacaze, PhD,
Head of the Public Health Genomics Program at Monash University, one of the
challenges in interpreting whole-genome data in order to diagnose disease is
“discriminating rare candidate disease-causing variants from the large numbers
of benign variants unique to each individual. Reference populations are
powerful filters,” he noted in the MGRB paper.
The MGRB database provides just such a powerful reference
population, giving researchers who are studying specific diseases a tool for
comparison.
Other Studies into Heathy Aging
Other initiatives to create datasets of genome information
for specific populations also are underway. The Scripps
Translational Science Institute (STSI) in La Jolla, Calif., has been
studying healthy aging since 2007. That’s when STSI launched the Wellderly Study,
according to a news
release. As of 2016, they had sequenced the genomes of 600 study
participants, as well as 511 samples for comparison from a study being conducted
separately by the Inova Translational Medicine Institute, a paper in Nature noted.
Another effort being conducted in China involves a database
called PGG.Population.
These researchers seek to “create a comprehensive depository of geographic and
ethnic variation of human genome, as well as a platform bringing influence on
future practitioners of medicine and clinical investigators,” according to
their 2018 paper published in Nucleic Acids
Research.
In this case, rather than identifying common genomic
variants among a specific population, such as the healthy elderly, the
researchers are working to understand how genetic variations are distributed
among specific populations. “The PGG.Population database documents 7,122
genomes representing 356 global populations from 107 countries and provides
essential information for researchers to understand human genomic diversity and
genetic ancestry,” wrote the researchers.
Each of these disparate datasets represents paths of
investigation that could lead to a better understanding of personal and public health.
As technologies continue to develop that enable scientists to sift through the
massive amount of WGS data being generated, a clearer picture of what healthy
aging at the genetic level looks like will likely emerge.
Precision medicine is leading to precision public health,
and clinical pathology laboratories are important parts of the public health
puzzle.